This post was originally published on this site
This year, celebrity gossip, a national shortage and eyebrow-raising clinical trials made household names of weight-loss and diabetes drugs like Ozempic, Wegovy and Mounjaro.
The buzzy drugs belong to a class of powerful medications that can manage blood sugar levels and drastically reduce body weight — a hot property that kicked them into the mainstream. This spring, even WeightWatchers got on board, acquiring a virtual clinic that offers prescriptions for the popular drugs.
The medications’ ever-expanding reach might explain why many people in the United States are having trouble filling prescriptions. From 2020 to 2022, the number of prescriptions for these drugs quadrupled — up to roughly 9 million in the final months of 2022, according to one analysis. In 2023, the U.S. Food and Drug Administration included both Ozempic and Wegovy on its drug shortages list.
And demand may continue to rocket up. Data from clinical trials and other studies suggest these drugs can improve cardiovascular health and perhaps even help treat addiction (SN: 8/30/23).
The FDA approved Ozempic for type 2 diabetes in 2017, and now new, potentially more potent and easier-to-produce versions are in the pipeline, says Susan Yanovski, a physician and nutrition specialist at the National Institute of Diabetes and Digestive and Kidney Diseases in Bethesda, Md. “I’ve been doing this for more than 30 years now, and I have not seen this degree of excitement.”
It’s the first time doctors have had obesity drugs that work so well, she says, approaching weight-loss levels previously seen only with bariatric surgery. But, Yanovski cautions, “it’s still early days.”
Amid the hubbub, a fresh influx of clinical trial data has opened a Pandora’s box of questions. How exactly do the drugs work? Who should take them? For how long? What’s the full range of side effects? “We’ve got a lot of research to do,” Yanovski says.
Semaglutide belongs to a powerful class of drugs
Ozempic is the brand name for the drug semaglutide; Wegovy, also semaglutide, has a higher maximum dose and is approved for weight loss. Semaglutide mimics a gut hormone, GLP-1, that’s secreted after people eat. When given a high dose weekly, people without diabetes can lose about 15 percent of their body weight, on average, after nearly 16 months. Scientists think the drug acts on the body and the brain, making people feel full and muffling food cravings.
Yet semaglutide may have an even more dramatic action — saving lives, scientists suggested November 11 in Philadelphia at the American Heart Association meeting. Weekly injections of the drug lowered the risk of heart attacks, strokes and death due to cardiovascular disease in some adults, Cleveland Clinic cardiologist A. Michael Lincoff reported (SN: 11/15/23). The trial targeted people who are overweight or obese who have high cardiovascular risk but not diabetes.
That’s important because it wasn’t clear until now that these patients would see heart benefits, says Tiffany Powell-Wiley, a cardiologist and epidemiologist at the National Heart, Lung and Blood Institute in Bethesda. The find “really opens up the number of patients that we can treat with semaglutide,” she says. Powell-Wiley notes, though, that no single drug — even a powerful one — can fix the many factors that lead to the development of obesity.
Still, pharmaceutical companies are racing to investigate new, improved relatives of semaglutide. Some of these drugs mimic multiple gut hormones rather than just one. One such molecule, tirzepatide (brand name Mounjaro), mimics both GLP-1 and the gut hormone GIP. The FDA approved tirzepatide for treating type 2 diabetes last year and for treating obesity in November, under the brand name Zepbound. The drug seems to cause even more weight loss than semaglutide, Yanovski says.
In demand
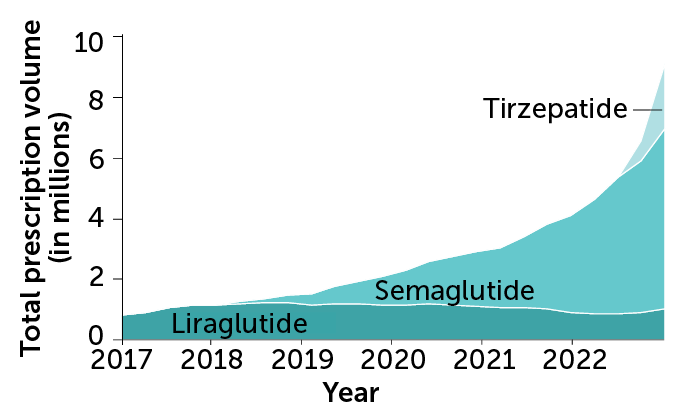
Over the last few years, prescriptions for diabetes and weight-loss drugs have skyrocketed in the United States. Semaglutide and a drug called liraglutide (approved in 2014) both mimic the gut hormone GLP-1. Semaglutide (sold as Ozempic) was approved to treat type 2 diabetes in December 2017 and for obesity (sold as Wegovy) in June 2021. Tirzepatide, which mimics GLP-1 plus the gut hormone GIP, was approved to treat type 2 diabetes (under the name Mounjaro) in May 2022.
GLP-1 prescription volume in the United States by drug, 2017–2022

Another drug in development could one-up even tirzepatide. Retatrutide simulates three gut hormones: GLP-1, GIP and glucagon. People treated with a high dose lost an average of 24 percent of their body weight after nearly a year of treatment, a small clinical trial reported this year.
The full roster of these drugs, what they do and where they stand in the approval process makes for a dizzying array of information. But an assortment of options may pay off, Yanovski says. “We really need a variety of drugs … so that we can match the right treatment to the right patient.”
For some people, the benefits of weight-loss drugs outweigh the risks
But like any medication, Yanovski cautions, these drugs come with side effects. Semaglutide can cause nausea, diarrhea, vomiting, stomachache and constipation, among other ailments. Large amounts of rapid weight loss can also spur gallbladder disease, a complication sometimes seen after bariatric surgery. And these medications aren’t melting away only fat. When people rapidly lose lots of weight, they can also lose muscle mass, a particular concern for older patients, Yanovski says.
As these drugs roll out into larger populations of people, rare side effects not seen in clinical trials will also emerge. One recent study found that people using semaglutide or a related drug for weight loss had an increased risk of serious gastrointestinal conditions, including inflammation of the pancreas and bowel blockages, compared with people using a different type of weight-loss drug.
And patients will probably need to take these medications long term or risk gaining the weight back. “This is not a flaw in the medications; this is how medications work,” Yanovski says. If you stop taking cholesterol-lowering meds, for instance, your cholesterol may shoot up.
But the drugs’ high cost (Wegovy’s list price is about $1,350 per month and insurance coverage varies) puts even short-term use out of reach for many people. The cost can exacerbate health disparities and drive people to hunt for altered versions on the internet. Though these drugs may be cheaper, Yanovski says, they’re not FDA-approved and could be counterfeit.
She hopes to see people with obesity, particularly those with medical complications, gain better access to the approved drugs and in settings where they can be monitored by their doctors to ensure that the benefits outweigh the risks.
Those without a true need for the drugs probably should avoid them, Yanovski says. They’re “serious medications for a serious disease,” she says. “I think the buzz that these are some kind of miracle cure for obesity, or that you should take these medications just because you want to lose that stubborn 10 pounds, is overhyped.”