Jan. 30, 2025 – Singer and actor overcame drug addiction and homelessness to collaborate with everyone from the Rolling Stones and Metallica to Jean-Luc Godard. Her six-decade career marked her out as one of the UK’s most versatile and characterful singer-songwriters.
President Donald Trump ratcheted up his administration’s reversal of transgender rights on Tuesday with an executive order that seeks to intervene in parents’ medical decisions by prohibiting government-funded insurance coverage of puberty blockers or surgery for people under 19.
Trump’s order, titled “Protecting Children From Chemical and Surgical Mutilation,” is certain to face legal challenges and would require congressional or regulatory actions to be fully enacted. But transgender people and their advocates are concerned it will nonetheless discourage prescriptions and medical procedures they consider to be lifesaving in some cases, while complicating insurance coverage for gender-affirming care.
“It can’t be understated how harmful this executive order is, even though it doesn’t do anything on its own,” said Andrew Ortiz, a senior policy attorney at the Transgender Law Center. “It shows where the administration wants to go, where it wants the agencies to put their efforts and energies.”
The order is one of several Trump has issued, less than two weeks since taking office, that target the trans community. He has directed his administration to recognize only the male and female sex — and to abandon the term “gender” altogether. He ordered the State Department to issue passports identifying Americans only by their genders assigned at birth. He has encouraged the Justice Department to prosecute teachers and other school officials who help trans children transition, including by using their preferred names. And he signed an order that’s expected to lead to transgender people being banned from military service.
“We’re terrified. We cry every day. Hurting my family and my kid is winning politics for Republicans right now,” said the parent of a transgender child who lives in Missouri and asked not to be identified for fear of being targeted. “Every bone in my body is telling me I can’t keep my child safe from my government anymore, I can’t keep my family safe.”
About 300,000 American children ages 13-17 identify as transgender, according to the Williams Institute at the UCLA School of Law, which researches sexual orientation and gender identity law and public policy. But the number who seek gender-affirming care is believed to be far fewer. An examination by Reuters and Komodo Health of about 330 million health insurance claims filed from 2017 to 2021 found that fewer than 15,000 patients ages 6 to 17 with a diagnosis of gender dysphoria had received gender-affirming hormone therapy and fewer than 5,000 had started puberty-blocking medications — though the annual number of such patients more than doubled over the five-year span.
Trump’s order seeking to disrupt insurance coverage for young people, the Williams Institute said in a brief, “will likely at least limit the availability of gender-affirming care or make it more difficult to access in the short term and could increase risk for both providers and recipients of the care.”
Much of what the order calls for would require rule changes or other federal guidance, which can take weeks to months. Though it is mostly directed toward government health insurance programs, the order could have private-sector implications, too, and is likely to face litigation from states or advocacy organizations.
Specifically, the directive intends to limit insurance coverage for hormonal or surgical treatments that help young people transition.
Subscribe to California Healthline’s free Daily Edition.
It directs the secretary of the Department of Health and Human Services to “take all appropriate steps” to end insurance coverage of such treatments. It specifically names several government programs such as Tricare, which serves the military and its dependents; Medicare and Medicaid; federal and postal health benefit programs; and the Foreign Service Benefit Plan.
“The aim here is clearly targeted at federally funded plans, such as Medicare and Medicaid, but there’s a lack of clarity as to whether it would impact other plans, such as exchange plans, where essential health benefits are required,” said Lindsey Dawson, director of LGBTQ Health Policy at KFF, the health policy research, polling, and news organization that includes KFF Health News.
State Medicaid programs vary widely in their rules around transgender care, with a variety of limits or restrictions on what types of care can be covered for minors in just over half the states, according to a map provided by the Colorado-based Movement Advancement Project, a nonprofit think tank.
While little is likely to happen immediately from the order — one of more than 100 issued by the president since his inauguration last week — it could, nonetheless, have a chilling effect on medical professionals.
The order directs the Department of Justice to work with Congress to promote legislation that would allow children and parents a “private right of action” — the ability to file a lawsuit — against medical professionals who provide transgender care.
And the Justice Department was also directed to consider the application of existing laws to those who provide or promote access to gender care.
In addition, one section of the order directs agencies to “take appropriate steps to ensure that institutions receiving Federal research or education grants end the chemical and surgical mutilation of children,” a move that could affect hospitals or medical schools.
Julian Polaris, a partner at the consulting firm Manatt, said the order “displays the federal government’s willingness to use federal programs to restrict access to disfavored services even to providers and patients outside those federal programs.”
The move drew immediate criticism from groups supporting LBGTQ+ people’s rights.
“It is unconscionable that less than 24 hours after trying to take away Head Start programs and school meals for kids, President Trump issued an order demonizing transgender youth and spreading dangerous lies about gender-affirming care,” Alexis McGill Johnson, president and CEO of Planned Parenthood Federation of America, wrote in a press release.
Because it defines “youths” as those under age 19, the order would apply the directives to medical treatments provided to 18-year-olds, who otherwise are considered adults in making legal choices, voting, or serving in the military.
“There’s also just a problem with not seeing young people as capable in making decisions around their health and their futures, and so blurring that line and trying to move it up and taking more control over more people is obviously concerning,” Ortiz said. “But having the line hard at 18 also doesn’t make it any better.”
Ortiz noted that the order contains misinformation about medical care for young people who are transitioning and targets a small subset of U.S. residents: transgender youths in families that can access and afford gender-affirming care.
“That should be concerning to everybody,” he said, “that they are pulling out populations to target, to say that, ‘We don’t think that you deserve access to best-practice medical care.’”
Trump’s order explained that the action was necessary because such medical treatment could cause young people to regret the move later, once they “grasp the horrifying tragedy that they will never be able to conceive children of their own or nurture their children through breastfeeding.”
KFF Health News Midwest correspondent Bram Sable-Smith contributed to this report.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
During her annual OB-GYN visit, Callie Anderson asked about getting off the birth control pill.
“We decided the best option for me was an IUD,” she said, referring to an intrauterine device, a long-acting, reversible type of birth control.
Anderson, 25, of Scranton, Pennsylvania, asked her doctor how much it might cost. At the time, she was working in a U.S. senator’s local office and was covered under her father’s insurance through a plan offered to retired state police.
“She told me that IUDs are almost universally covered under insurance but she would send out the prior authorization anyway,” Anderson said.
She said she heard nothing more and assumed that meant it was covered.
After waiting months for an appointment, Anderson had the insertion procedure last March. She paid $25, her copay for an office visit, and everything went well.
“I was probably in the room itself for less than 10 minutes, including taking clothes on and off,” she said.
Subscribe to California Healthline’s free Daily Edition.
The Medical Procedure
According to Planned Parenthood, IUDs and implantable birth control represented nearly 25% of its contraceptive services provided from October 2021 to September 2022, per the latest data available.
There are two types of IUDs: copper, which Planned Parenthood says can protect against pregnancy for up to 12 years, and hormonal, which can last from three to eight years depending on the brand. Hormonal IUDs can prevent ovulation, and both types affect the movement of sperm, designed to stop them from reaching an egg.
A physician or other practitioner uses a tube to insert the IUD, passing it through the cervix and releasing it into the uterus.
Doctors often recommend over-the-counter drugs for insertion pain, a concern that prompts some patients to avoid IUDs. Last year, federal health officials recommended doctors discuss pain management with patients beforehand, including options such as lidocaine shots and topical anesthetics.
The Final Bill
$14,658: $117 for a pregnancy test, $9,862 for a Skyla IUD, $4,057 for “clinic service,” plus $622 for the doctor’s services.
The Billing Problem: A ‘Grandfathered’ Plan
Anderson got a rare glimpse of what can happen when insurance doesn’t cover contraception.
But Anderson’s plan doesn’t have to comply with the ACA. That’s because it’s considered a “grandfathered” plan, meaning it existed before March 23, 2010, when President Barack Obama signed the ACA into law, and has not changed substantially since then.
It’s unclear how many Americans have such coverage. In its 2020 Employer Health Benefits survey, KFF estimated that about 14% of covered workers were still on “grandfathered” plans.
Anderson said she didn’t know that the plan was grandfathered — and that it did not cover IUDs — until she contacted her insurer after it denied payment. Her doctor with Geisinger, a nonprofit health system in Pennsylvania, was in-network.
“My understanding was Geisinger would reach out to insurance and if there was an issue, they would tell me,” she said.
Mike McCullen, a Geisinger spokesperson, said in an email to KFF Health News that with most insurance plans, “prior authorization is not required for placing birth control devices, however, some insurers may require prior authorization for the procedure.”
He did not specify whether it is the health system’s policy to seek such authorizations for IUDs, nor did he comment on the amount charged.
The Pennsylvania State Troopers Association, which offers some retirees the plan that covered Anderson, did not respond to requests for comment. Highmark Blue Cross Blue Shield, the insurer, referred questions to the state.
Dan Egan, communications director for the state’s Office of Administration, confirmed in an email that the insurance plan is a grandfathered plan “for former Pennsylvania State Troopers Association members who retired prior to January 13, 2018.”
A benefit handbook for the plan identifies it as grandfathered and lists a variety of excluded services. Among them are “contraceptive devices, implants, injections and all related services.”
The $14,658 bill, an amount that typically would be negotiated down by an insurer, was solely Anderson’s responsibility.
“Fourteen thousand dollars is astronomical. I’ve never heard of anything that high” for an IUD, said Danika Severino Wynn, vice president for care and access at the Planned Parenthood Federation of America.
Costs for IUDs vary, depending on the type, where the patient lives, insurance status, the availability of financial assistance, and additional medical factors, Severino Wynn said.
She said most insurers cover the devices, but coverage can vary, too. For instance, some cover only certain types or brands of contraceptives. Generally, an IUD insertion costs $500 to $1,500, she added.
Many providers, including Planned Parenthood, have sliding-scale rates based on income or can set up payment plans for cash-paying or underinsured patients, she said.
According to FAIR Health, a cost estimation tool that uses claims data, an uninsured patient in the Scranton area could expect to be charged $1,183 for an IUD insertion done at an ambulatory surgery center or $4,319 in a hospital outpatient clinic.
The Affordable Care Act requires health plans to cover preventive care, including contraception. But “grandfathered” plans — those that existed before the act became law and have not changed substantially since — do not have to comply with the ACA. Anderson says she didn’t know she had such a plan until her insurer denied payment for her IUD.(Jason Ardan for KFF Health News)
The Resolution
Anderson texted and called her insurer and Geisinger multiple times, spending hours on the phone. “I am appalled that no one at Geisinger checked my insurance,” she wrote in one message with staff at her doctor’s office.
She said she felt rebuffed when she asked billing representatives about financial assistance, even after noting the bill was more than 20% of her annual income.
“I wasn’t in therapy at the time, but at the end of this I ended up going to therapy because I was stressed out,” she said. The billing office, she said, “told me that if I didn’t pay in 90 days, it would go to collections, and that was scary to me.”
Eventually, she was put in touch with Geisinger’s financial assistance office, which offered her a self-pay discount knocking $4,211 off the bill. But she still owed more than she could afford, Anderson said.
The final offer? She said a representative told her by phone that if she made one lump payment, Geisinger would give her half off the remaining charges.
She agreed, paying $5,236 in total.
The Takeaway
It’s always best to read your benefit booklet or call your insurer before you undergo a nonemergency medical procedure, to check whether there are any exclusions to coverage. In addition, call and speak with a representative. Ask what you might owe out-of-pocket for the procedure.
While it can be hard to know whether your plan is grandfathered under the ACA, it’s worth checking. Ask your insurance plan, your employer, or the retiree benefits office that offers your coverage. Ask where the plan deviates from ACA rules.
With birth control, “sometimes you have to get really specific and say, ‘I’m looking for this type of IUD,’” Severino Wynn said. “It’s incredibly hard to be an advocate for yourself.”
Most insurance plans offer online calculators or other ways to learn ahead of time what patients will owe.
Be persistent in seeking discounts. Provider charges are almost always higher than what insurers would pay, because they are expected to negotiate lower rates.
Bill of the Month is a crowdsourced investigation by KFF Health News and The Washington Post’s Well+Being that dissects and explains medical bills. Since 2018, this series has helped many patients and readers get their medical bills reduced, and it has been cited in statehouses, at the U.S. Capitol, and at the White House. Do you have a confusing or outrageous medical bill you want to share? Tell us about it!
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
El presidente Donald Trump ha reforzado la decisión de su gobierno de revertir los derechos de las personas transgénero. Una orden ejecutiva del 28 de enero busca intervenir en las decisiones médicas de los padres prohibiendo que seguros de salud financiados por el gobierno cubran bloqueadores de la pubertad o cirugías para menores de 19 años.
La orden de Trump, titulada “Proteger a los niños de la mutilación química y quirúrgica”, seguramente enfrentará batallas legales, y requerirá medidas legislativas o cambios reglamentarios para implementarse por completo.
Sin embargo, las personas transgénero y sus defensores temen que la medida desaliente el uso de medicamentos y los tratamientos médicos que, en algunos casos, consideran vitales, además de complicar la cobertura de los procedimientos de afirmación de género.
“No se puede subestimar lo perjudicial que es esta orden ejecutiva, incluso aunque no tenga efecto inmediato por sí sola”, dijo Andrew Ortiz, abogado senior de políticas en el Transgender Law Center. “Muestra hacia dónde quiere ir la administración y en qué áreas pretende que las agencias enfoquen sus esfuerzos y energías”.
La orden es una de las varias normas dirigidas a la comunidad trans que Trump ha emitido a menos de dos semanas de asumir el cargo. El presidente ha ordenado a su administración que solo reconozca los sexos masculino y femenino, y que abandone por completo el término “género”.
También instruyó al Departamento de Estado para que emita pasaportes que solo identifiquen a los ciudadanos estadounidenses según el género asignado al nacer.
Y alentó al Departamento de Justicia para que procese a los profesores y otros funcionarios escolares que ayuden a los niños trans a hacer su transición, aunque solo se limiten a permitirles usar el nombre que prefieran. Y ha firmado una orden que llevaría a prohibir que las personas trans formen parte de las Fuerzas Armadas.
“Estamos aterrados. Lloramos todos los días. En este momento, para los republicanos es una victoria política lastimar a mi familia y a mi hijo”, dijo el padre de un niño transgénero que vive en Missouri, y pidió no ser identificado por miedo a convertirse en blanco de ataques. “Cada fibra de mi ser me dice que ya no puedo proteger a mi hijo de mi gobierno, ni puedo mantener a mi familia a salvo”, agregó.
Cerca de 300.000 niños estadounidenses de entre 13 y 17 años se identifican como transgénero, según el Williams Institute de la Facultad de Derecho de la UCLA, que investiga las leyes y políticas públicas sobre orientación sexual e identidad de género.
Pero, se cree que el número de quienes buscan atención de afirmación de género es mucho menor.
Un análisis de Reuters y Komodo Health sobre aproximadamente 330 millones de solicitudes de seguros de salud presentadas entre 2017 y 2021 encontró que menos de 15.000 pacientes de entre 6 y 17 años con un diagnóstico de disforia de género habían recibido terapia hormonal de afirmación de género, y menos de 5.000 habían comenzado a tomar bloqueadores de la pubertad.
Aun así, el número anual de estos pacientes se incrementó en más del doble en ese período de cinco años.
Al buscar interrumpir la cobertura para los jóvenes, la orden de Trump “probablemente, como mínimo, limitará la disponibilidad de la atención de afirmación de género o hará que sea más difícil acceder a ella a corto plazo. También podría aumentar el riesgo tanto para los proveedores como para los pacientes”, aseguró en un informe el Williams Institute.
La implementación de la orden ejecutiva podría tardar semanas o meses porque gran parte de lo que exige requeriría cambios normativos o nuevas directrices federales.
Aunque está dirigida principalmente a programas de salud del gobierno, la orden también podría tener implicaciones para el sector privado y es probable que enfrente litigios por parte de los estados o grupos de defensa.
Específicamente, la directiva busca limitar la cobertura para tratamientos hormonales o quirúrgicos destinados a ayudar a los jóvenes en su transición.
La directiva ordena al secretario del Departamento de Salud y Servicios Humanos (HHS) que tome “todas las medidas apropiadas” para eliminar la cobertura de estos tratamientos. Menciona específicamente varios programas gubernamentales como Tricare, que atiende al personal del ejército y sus familias; Medicare y Medicaid; los programas de atención de la salud para trabajadores y jubilados del gobierno federal y del servicio postal, y el Foreign Service Benefit Plan, para empleados del Servicio Exterior.
“El objetivo aquí está claramente dirigido a los planes financiados por el gobierno federal, como Medicare y Medicaid, pero no está claro si la orden afectaría a otros planes, como los del mercado de seguros en los que se garantiza la cobertura de ciertos servicios de salud considerados esenciales”, explicó Lindsey Dawson, directora de Políticas de Salud LGBTQ en KFF.
Los programas estatales de Medicaid tienen reglas muy diferentes sobre la atención médica para personas transgénero. En poco más de la mitad de los estados, existen límites o restricciones sobre los tipos de tratamientos que pueden cubrirse para los menores, según un mapa realizado por el Movement Advancement Project, un grupo de investigación sin fines de lucro con sede en Colorado.
Aunque es poco probable que la orden tenga un impacto inmediato —es solo una de las más de las 100 que el presidente ha firmado desde que asumió el cargo—, podría hacer que muchos médicos se sientan intimidados o temerosos de brindar este tipo de atención.
La orden instruye al Departamento de Justicia para que trabaje con el Congreso en la elaboración de una legislación que permita a los niños y sus padres una “acción de derecho privado” —esto es, la capacidad de presentar una demanda— contra los profesionales médicos que brinden atención a personas transgénero.
Además, se le indicó que considere la aplicación de las leyes existentes a quienes brinden o faciliten el acceso a la atención de género.
Otra sección de la orden les pide a las agencias que “tomen medidas para asegurarse de que las instituciones que reciban fondos federales para investigación o educación terminen con la mutilación química y quirúrgica de los niños”, lo que podría afectar a hospitales o escuelas de medicina.
Julian Polaris, un socio de la firma de consultoría Manatt, comentó que la orden “muestra que el gobierno federal está dispuesto a usar sus programas para restringir el acceso a servicios que desaprueba, incluso para médicos y pacientes que no estén dentro de esos programas federales”.
De inmediato, la medida recibió críticas de grupos defensores de los derechos de las personas LGBTQ+.
“Es inconcebible que, menos de 24 horas después de intentar eliminar programas de alimentación escolar y Head Start para niños, el presidente Trump emita una orden demonizando a los jóvenes transgénero y difundiendo mentiras peligrosas sobre la atención de afirmación de género”, manifestó en un comunicado de prensa Alexis McGill Johnson, presidenta y CEO de Planned Parenthood Federation of America.
Dado que la orden define a “jóvenes” como aquellos menores de 19 años, también afectaría las directrices de los tratamientos médicos proporcionados a los mayores de 18 años, quienes sin embargo son considerados adultos con derecho a tomar decisiones legales, votar o servir en el ejército.
“También es problemático no reconocer a los jóvenes como capaces de tomar decisiones sobre su salud y su futuro. Diluir esa línea y tratar de moverla hacia arriba para tener más control sobre más personas es, obviamente, preocupante”, dijo Andrew Ortiz. “Pero incluso fijar un límite estricto en los 18 años tampoco lo hace mejor”.
Ortiz señaló que la orden contiene información errónea sobre la atención médica para jóvenes en transición y se enfoca a un pequeño grupo de la población: los jóvenes transgénero cuyas familias pueden acceder y costear la atención de afirmación de género.
“Eso nos debería preocupar a todos”, concluyó, “porque están seleccionando poblaciones específicas para atacarlas y decirles que ‘no merecen acceso a una atención médica basada en las mejores prácticas’”.
Trump justificó la orden argumentando que el tratamiento médico para jóvenes trans podría llevar al arrepentimiento en el futuro, “cuando se den cuenta de la horrible tragedia de que nunca podrán concebir hijos propios ni amamantarlos”.
Bram Sable-Smith, corresponsal en el Medio Oeste de KFF Health News, colaboró con este artículo.
Esta historia fue producida por KFF Health News, conocido antes como Kaiser Health News (KHN), una redacción nacional que produce periodismo en profundidad sobre temas de salud y es uno de los principales programas operativos de KFF, la fuente independiente de investigación de políticas de salud, encuestas y periodismo.
Robert F. Kennedy Jr., President Donald Trump’s nominee to lead the Department of Health and Human Services, came under sharp questioning from Democrats and some Republicans at his confirmation hearings this week before two Senate committees. Of particular interest were the doubts about Kennedy’s qualifications and past anti-vaccination positions raised by Sen. Bill Cassidy (R-La.), who is a physician — and, notably, a member of the Senate Finance Committee, which is expected to vote next week on whether to advance Kennedy’s nomination to the Senate floor.
Meanwhile, a federal government memo temporarily freezing a lot of federal grant and loan funding touched off confusion and recriminations at the new Trump administration for its sudden, sweeping actions.
This week’s panelists are Julie Rovner of KFF Health News, Sandhya Raman of CQ Roll Call, and Sarah Karlin-Smith of the Pink Sheet.
Panelists
Among the takeaways from this week’s episode:
During appearances before two Senate committees, Kennedy assured lawmakers he would follow science and defer to Trump’s policy preferences. But he also made mistakes that are notable for someone vying to lead the nation’s top health agency, such as confusing the Medicaid and Medicare programs.
As Kennedy’s second hearing concluded, it was not immediately clear whether he would earn the votes needed to be confirmed by the full Senate — especially as at least one key Republican, Cassidy, seemed less than convinced. If every Democrat and independent votes against him, Kennedy could lose just a few GOP votes and still be confirmed.
Much of the nation’s health system — alongside many, many other entities that rely on federal funding — experienced a kind of whiplash early this week, as the Trump administration’s Office of Management and Budget issued a memo freezing federal grants and loans until they could be reviewed for adherence to Trump’s priorities. A federal judge temporarily blocked the freeze from taking effect, and OMB revoked the memo — but the White House said Trump’s recent executive orders affecting funding “remain in full force and effect, and will be rigorously implemented.”
In other Trump administration news, Trump fired a slew of inspectors general late last week — including the one who oversees HHS and the nation’s health system. And an executive order affecting health care for trans children has many parents and advocates on edge.
Also this week, Rovner interviews Nicholas Bagley, a University of Michigan law professor, who explains how the federal regulatory system is supposed to operate to make health policy.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
Robert F. Kennedy Jr.’s confirmation hearings for secretary of Health and Human Services are happening Jan. 29 and Jan. 30, and KFF Health News reporters will be watching as the Senate Committee on Finance and the Senate Committee on Health, Education, Labor and Pensions ask Kennedy about everything from vaccines to abortion to Medicaid.
What are the biggest takeaways? What comes next? Tune in for a discussion with KFF Health News’ Arthur Allen, Phil Galewitz, and Julie Rovner on Thursday, Jan. 30, at 12:30 p.m. PT.
The Trump administration has intervened in the release of important studies on the bird flu, as an outbreak escalates across the United States.
One of the studies would reveal whether veterinarians who treat cattle have been unknowingly infected by the bird flu virus. Another report documents cases in which people carrying the virus might have infected their pet cats.
The studies were slated to appear in the official journal of the Centers for Disease Control and Prevention, the Morbidity and Mortality Weekly Report. The distinguished journal has been published without interruption since 1952.
Its scientific reports have been swept up in an “immediate pause” on communications by federal health agencies ordered by Dorothy Fink, the acting secretary of the Department of Health and Human Services. Fink’s memo covers “any document intended for publication,” she wrote, “until it has been reviewed and approved by a presidential appointee.” It was sent on President Donald Trump’s first full day in office.
That’s concerning, former CDC officials said, because a firewall has long existed between the agency’s scientific reports and political appointees.
“MMWR is the voice of science,” said Tom Frieden, a former CDC director and the CEO of the nonprofit organization Resolve to Save Lives.
“This idea that science cannot continue until there’s a political lens over it is unprecedented,” said Anne Schuchat, a former principal deputy director at the CDC. “I hope it’s going to be very short-lived, but if it’s not short-lived, it’s censorship.”
White House officials meddled with scientific studies on covid-19 during the first Trump administration, according to interviews and emails collected in a 2022 report from congressional investigators. Still, the MMWR came out as scheduled.
“What’s happening now is quite different than what we experienced in covid, because there wasn’t a stop in the MMWR and other scientific manuscripts,” Schuchat said.
Neither the White House nor HHS officials responded to requests for comment. CDC spokesperson Melissa Dibble said, “This is a short pause to allow the new team to set up a process for review and prioritization.”
News of the interruption hit suddenly last week, just as Fred Gingrich, executive director of the American Association of Bovine Practitioners, a group for veterinarians specializing in cattle medicine, was preparing to hold a webinar with members. He planned to disclose the results of a study he helped lead, slated for publication in the MMWR later that week. Back in September, about 150 members had answered questions and donated blood for the study. Researchers at the CDC analyzed the samples for antibodies against the bird flu virus, to learn whether the veterinarians had been unknowingly infected earlier last year.
Although it would be too late to treat prior cases, the study promised to help scientists understand how the virus spreads from cows to people, what symptoms it causes, and how to prevent infection. “Our members were very excited to hear the results,” Gingrich said.
Like farmworkers, livestock veterinarians are at risk of bird flu infections. The study results could help protect them. And having fewer infections would lessen the chance of the H5N1 bird flu virus evolving within a person to spread efficiently between people — the gateway to a bird flu pandemic.
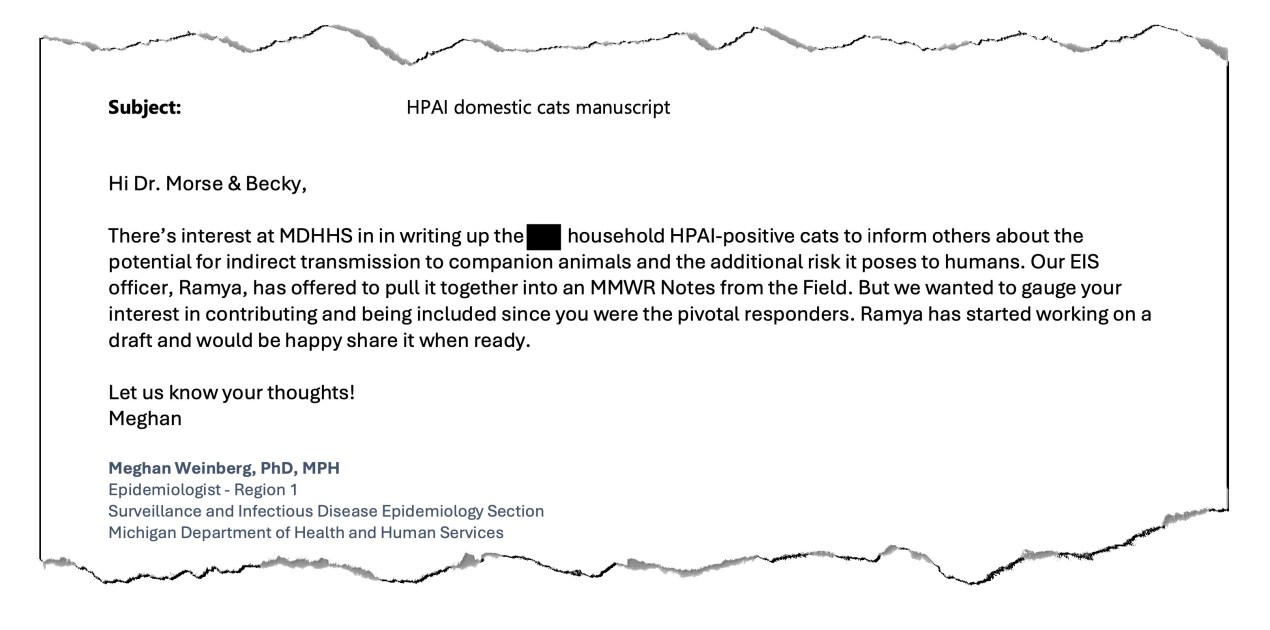
In a July 22 email obtained by KFF Health News, an epidemiologist at the Michigan health department suggests publishing a report about people who potentially spread the bird flu virus to their pet cats. The paper was accepted by the journal of the Centers for Disease Control and Prevention. But its publication is on hold because of a Trump administration order to pause communications. (Screenshot by KFF Health News)
At least 67 people have tested positive for the bird flu in the U.S., with the majority getting the virus from cows or poultry. But studies and reporting suggest many cases have gone undetected, because testing has been patchy.
Just before the webinar, Gingrich said, the CDC informed him that because of an HHS order, the agency was unable to publish the report last week or communicate its findings. “We had to cancel,” he said.
Another bird flu study slated to be published in the MMWR last week concerns the possibility that people working in Michigan’s dairy industry infected their pet cats. These cases were partly revealed last year in emails obtained by KFF Health News. In one email from July 22, an epidemiologist pushed to publish the group’s investigation to “inform others about the potential for indirect transmission to companion animals.”
Jennifer Morse, medical director at the Mid-Michigan District Health Department and a scientist on the pending study, said she got a note from a colleague last week saying that “there are delays in our publication — outside of our control.”
Veterinarians who treat cattle await a report that could help protect them from infection with the bird flu. This photo of a runny cow nose was taken by a veterinarian working on a farm with an outbreak. (They provided it on the condition of anonymity because of concerns about reputational damage.)
A person close to the CDC, speaking on the condition of anonymity because of concerns about reprisal, expected the MMWR to be on hold at least until Feb. 6. The journal typically posts on Thursdays, and the HHS memo says the pause will last through Feb. 1.
“It’s startling,” Frieden said. He added that it would become dangerous if the reports aren’t restored. “It would be the equivalent of finding out that your local fire department has been told not to sound any fire alarms,” he said.
In addition to publishing studies, the MMWR keeps the country updated on outbreaks, poisonings, and maternal mortality, and provides surveillance data on cancer, heart disease, HIV, and other maladies. Delaying or manipulating the reports could harm Americans by stunting the ability of the U.S. government to detect and curb health threats, Frieden said.
The freeze is also a reminder of how the first Trump administration interfered with the CDC’s reports on covid, revealed in emails detailed in 2022 by congressional investigators with the House Select Subcommittee on the Coronavirus Crisis. That investigation found that political appointees at HHS altered or delayed the release of five reports and attempted to control several others in 2020.
In one instance, Paul Alexander, then a scientific adviser to HHS, criticized a July 2020 report on a coronavirus outbreak at a Georgia summer camp in an email to MMWR editors, which was disclosed in the congressional investigation. “It just sends the wrong message as written and actually reads as if to send a message of NOT to re-open,” he wrote. Although the report’s data remained the same, the CDC removed remarks on the implications of the findings for schools.
Later that year, Alexander sent an email to then-HHS spokesperson Michael Caputo citing this and another example of his sway over the reports: “Small victory but a victory nonetheless and yippee!!!”
Schuchat, who was at the CDC at the time, said she had never experienced such attempts to spin or influence the agency’s scientific reports in more than three decades with the agency. She hopes it won’t happen again. “The MMWR cannot become a political instrument,” she said.
Gingrich remains hopeful that the veterinary study will come out soon. “We’re an apolitical organization,” he said. “Maintaining open lines of communication and continuing research with our federal partners is critical as we fight this outbreak.”
Oh, look an entire investigation, of course partly by shatterproof, looking at where the settlement funds are going, and where they should go. Not one mention of pain patients as forgotten victims. Because we’ve actually been erased from the entire thing. https://t.co/LsHFs9tFwu
What should not be overlooked by those interested in solving this public health crisis (legislators, health department officials, and law enforcement and court system leaders) is that such downstream efforts, even when supported by unimaginable funding, does little to prevent those pushing our citizens into the quicksand of individual, family, and community destruction and death. Certainly, such mitigating and treatment programs and services are needed, but little attention is given to rooting out the root cause of the opioid/fentanyl epidemic.
It is easy and popular to damn the corporation, but it takes courage, real work, and much risk to confront Mexico’s drug cartels, Mexico’s government officials, the Chinese Communist Party, and any of their ostensible “leaders.” Furthermore, it is embarrassing to have to confront our own public officials, from the president on down, to stop aiding and abetting this carnage!
If no serious action is taken to work on upstream causes of our opioid crisis, no amount of lifeguarding and posting of warning signs will prevent bodies from struggling in this rip current of drug addiction. The silence and omission of any action from those who have taken the oath to defend and protect the public is creating a moral hazard for all citizens. Consequently, many more people will die, with nary a word against who is pushing them to such destruction.
— Stephen Gambescia, Philadelphia
A retired assistant surgeon general and epidemiologist weighed in on X about an article on the nation’s shortage of primary care providers:
Misdiagnosis. Young people choosing not to become primary care physicians after leaving med school will not be fixed by free tuition for the highest paid profession in America. Fix govt incentives about graduate medical education & reimbursementhttps://t.co/tPgeFVrzql
Osteopaths Have Big Hand in Filling Primary Care Needs
I appreciate Felice J. Freyer’s insightful Jan. 13 article, “Can Medical Schools Funnel More Doctors Into the Primary Care Pipeline?” As an osteopathic physician and medical educator, I can confidently answer this question with a resounding “Yes!” Osteopathic medical schools have long been at the forefront of this issue by emphasizing core principles of primary care as they train future physicians, a mission embedded in our philosophy since 1874.
Osteopathic medicine is founded on four key tenets that emphasize the interconnected nature of the body, mind, and spirit and the importance of whole-person care. These tenets have guided many of this country’s nearly 150,000 DOs (doctors of osteopathic medicine) into primary care roles. More than half of DOs enter residencies in the primary care specialties of family medicine, internal medicine, and pediatrics.
As mentioned in the article, “Many medical students start out expressing interest in primary care. Then they end up at schools based in academic medical centers, where students become enthralled by complex cases in hospitals, while witnessing little primary care.” This is a major part of the problem. Most Americans, more than 80%, will never be treated in a large academic medical center. Osteopathic medical schools have flipped the script.
Osteopathic medical schools, as well as some newer MD-granting schools, employ a community-based distributed education model, training students in settings such as rural clinics, community health centers, and physician offices where they will encounter underserved populations benefiting from primary care treatment. Training in underserved areas makes medical students almost three times as likely to stay in those areas to practice, and four times as likely to practice primary care in those locations.
I thank Freyer for shining a spotlight on the essential role of primary care and the contributions of osteopathic medicine. The osteopathic medical education community remains committed to working to ensure that underserved communities receive the care they deserve, and that primary care continues to thrive as the backbone of our health care system.
— Robert A. Cain, CEO and president of the American Association of Colleges of Osteopathic Medicine, Bethesda, Maryland
A family doctor and teacher shared the article on X:
The answer is that they can, but they won’t try. Financial and public good incentives for schools are not there. Can Medical Schools Funnel More Doctors Into the Primary Care Pipeline? https://t.co/REsfJtfmmh via @kffhealthnews
According to 42 U.S. Code § 300aa–22, vaccine producers have immunity in civil court. It reads: “No vaccine manufacturer shall be liable in a civil action for damages arising from a vaccine-related injury or death associated with the administration of a vaccine after October 1, 1988, solely due to the manufacturer’s failure to provide direct warnings to the injured party (or the injured party’s legal representative) of the potential dangers resulting from the administration of the vaccine manufactured by the manufacturer.”
And there is only one federal National Vaccine Injury Compensation Program, also known as “vaccine court,” to hear all vaccine-related injury cases involving children. And its case backlog is at least a decade long.
In everything else, when a product or service causes harm, there is accountability through the process of civil suits. What other manufacturer of a product has such legal immunity?
The issue with this is there is no true measure to create accountability with vaccine products. And vaccine makers aren’t required to display ingredient labels. So, we may be injecting our children with unknown substances, from a manufacturer who has no judicial accountability if harm results from the use of the product.
Now, what parent wants to subject their child to this? This is a big deterrent to parents vaccinating their children. Emotional appeal will not dissuade parents, but correcting this legal fallacy will.
— Alesia Wright, Tulsa, Oklahoma
An Indiana dad expressed his opinion on X:
Indiana’s childhood vaccination rates have dropped significantly since the pandemic too. Some people are just going to have to learn the hard way, apparently. Sad that the only way that happens, however, is by gambling with their kid’s health.https://t.co/S9UgXAlAc6
As a retired primary care physician, I was often frustrated that my management of complex medical conditions was reimbursed at lower rates due to a required treatment code (“Perspective: Removing a Splinter? Treating a Wart? If a Doctor Does It, It Can Be Billed as Surgery,” Dec. 13). Blaming the physician for the discrepancy is inappropriate. The Centers for Medicare & Medicaid Services has strict regulations on billing. We are mandated to code per the regulations. We cannot give “discounts” for procedures. To do so would be problematic in the bizarre catch-22 world of Medicare billing. We are mandated to report our services accurately using only the codes available. To do otherwise is considered fraud by Medicare. When a physician is accused of fraud, he/she is presumed guilty and pays significant financial penalties until innocence is proven. Even a murderer or thief has more rights in the judicial system.
Medicare determines the lowest reimbursement rate; the other carriers pay a higher rate based on that rate. If an individual physician accepts Medicare, he/she must accept that rate. Only a non-participating physician (not accepting Medicare) can offer a lower rate. The exception is if the service is provided at no cost. Should the patient demand the service be provided free?
I’m reminded of the plumber charging $100 to replace a washer: 10 cents for the washer and $99.90 to know how to replace it.