Pennsylvania is rolling out its new “Pennie” this fall: a state-run insurance exchange that officials say will save residents collectively millions of dollars on next year’s health plan premiums.
Since the Affordable Care Act’s marketplaces opened for enrollment in fall 2013, Pennsylvania, like most states, has used the federal www.healthcare.gov website for people buying coverage on their own.
But in a move defying the usual political polarization, state lawmakers from both parties last year agreed the cost of using the federal marketplace had grown too high and the state could do it for much less. They set up the Pennsylvania insurance exchange (nicknamed “Pennie”), designed to pass on expected savings to policyholders. Although the final rates for 2021 are not yet set, insurers have requested about a 3% average drop in premiums.
Pennsylvania is one of six states shifting in the next several years from the federal insurance exchange to run their own online marketplaces, which determine eligibility, assist with enrollment and connect buyers with insurance companies. They will join 12 states and the District of Columbia with self-contained exchanges.
The transitions come amid mounting evidence that state marketplaces attract more consumers, especially young adults, and hold down prices better than the federal exchange. They’ve also been gaining appeal since the Trump administration has cut the enrollment period on healthcare.gov and slashed funds for advertising and helping consumers.
State policymakers say they can run their own exchanges more cheaply and efficiently, and can better respond to residents’ and insurers’ needs.
“It comes down to getting more bang for your buck,” said Rachel Schwab, a researcher at Georgetown University’s Center on Health Insurance Reforms in Washington, D.C.
The importance of state-run exchanges was highlighted this year as all but one of them held special enrollment periods to sign up hundreds of thousands of people hurt financially by COVID-caused economic turmoil. The federal exchange, run by the Trump administration, refused to do so, although anyone who has lost workplace insurance is able to buy coverage anytime on either the state or federal exchange.
Like Pennsylvania, New Jersey expects to have its state-run exchange operational for the start of open enrollment on Nov. 1.
In fall 2021, New Mexico plans to launch its own marketplace and Kentucky is scheduled to fully revive its state-run exchange, which was dismantled by its Republican governor in 2015. Maine has also announced it will move to set up its own exchange, possibly in fall 2021.
Nationwide, about 11 million people get coverage through the state and federal exchanges, with more than 80% receiving federal subsidies to lower their insurance costs.
“Almost across the board, states with their own exchanges have achieved higher enrollment rates than their federal peers, along with lower premiums and better consumer education and protection,” according to a study published this month in the Journal of Health Politics, Policy and Law.
Controlling ‘Their Own Destiny’
Since 2014, states using the federal marketplaces have had a rise in premiums of 87% while state exchanges saw 47% growth, the study found.
In one key metric, from 2016 to 2019 the number of young enrollees in state exchanges rose 11.5%, while states using the federal marketplace recorded an 11.3% drop, a study by the National Academy for State Health Policy found.
Attracting younger enrollees, who tend to be healthy, is vital to helping the marketplaces spread the insurance risk to help keep premiums down, experts say.
When the Affordable Care Act was debated, Republicans and some Democrats in Congress were cautious about a one-size-fits-all approach to insurance and accusations about a federal takeover of health care. So the law’s advocates gave states more control over selling private health coverage. The law’s framers included a provision that allowed states to use millions in federal dollars to launch their own insurance exchanges.
Initially, 49 states took the money. But in 2011, conservative groups convinced Republican-controlled states that forgoing state-run exchanges would help undermine Obamacare.
As a result, most GOP-controlled states defaulted to the federal marketplace.
In the ensuing years, several states that had started their own marketplaces, such as Oregon, Nevada and Hawaii, reverted to the federal exchange because of technological problems. Nevada relaunched its exchange last fall.
“States want to control their own destiny, and the instability of healthcare.gov in the Trump administration has frustrated states,” said Joel Ario, managing director for the consulting firm Manatt Health Solutions and a former Obama administration official, who helped set up the exchanges. States running their own platform can use data to target enrollment efforts, he said.
An Effort to Hold Down Premium Increases
Marlene Caride, New Jersey commissioner of Banking and Insurance, said that “the beauty of [a state-based exchange] is we can tailor it to New Jersey residents and have the ability to help [them] when they are in dire need.”
About 210,000 New Jersey residents enrolled in marketplace health plans for this year.
New Jersey has been spending $50 million a year in user fees for the federal exchange. After startup costs, the state estimates, it will cost about $7.6 million a year to run its own exchange enrollment platform and $7 million a year for a customer service center.
Open enrollment on the New Jersey exchange — called Get Covered NJ — will run from Nov. 1 to Jan. 31.
Kentucky officials said insurers there were paying $15 million a year in user fees for healthcare.gov, a cost passed on to policyholders. When the state switches to its own operation, it plans to collect $5 million in its first year to cover the startup costs to revive its Kynect exchange and another $1 million to $2 million in annual administrative costs. So insurers will pay lower fees and those savings will help cut premium costs, said Eric Friedlander, secretary of the Kentucky Cabinet for Health and Family Services.
States using the federal marketplace this year paid either a 2.5% or 3% surcharge to the federal government on premiums collected.
In Pennsylvania, where about 330,000 residents buy coverage through an exchange plan, those fees accounted for $90 million a year. State officials estimate they can run their own exchange for about $40 million and will use the savings for a reinsurance program that pays insurers to help cover the cost of extremely expensive health care needed by some customers. Removing those costs from the insurers’ responsibility allows them to drop premiums by 5% to 10%, the state projects.
“When we talk about bringing something back to state control, that is a real narrative that can appeal to both sides of the aisle,” said Jessica Altman, the state’s insurance commissioner. “There is nothing political about making health insurance more affordable.” (Altman is the daughter of Drew Altman, CEO of KFF. KHN is an editorially independent program of KFF.)
Without the savings from running its own exchange, Pennsylvania would not have been able to come up with the more than $40 million needed for the reinsurance program, state officials said.
In addition, Pennsylvania has extended its enrollment period to run an extra month, until Jan. 15 (federal marketplace enrollment ends Dec. 15). Pennie also plans to spend three to four times the $400,000 that the federal government allocated to the state for navigators to help with enrollment, said Zachary Sherman, who heads Pennie.
“We think increased outreach and marketing will bring in a healthier population and broaden enrollment,” he said.
Thousands of letters stuffed with money flooded Jonas Salk’s mailbox the week after his polio vaccine was declared safe and effective in 1955. Everybody wanted his vaccine. Desperate parents clogged doctors’ phone lines in search of the precious elixir; drug companies and doctors diverted doses to the rich and famous.
Some of the first batches of the vaccine were disastrously botched, causing 200 cases of permanent paralysis. That barely dented public desire for the preventive. Marlon Brando even asked to play Salk in a movie.
Eight years later, with polio a fading threat, the first measles vaccines went on sale. Measles had killed more than 400 children the year before and caused permanent brain damage in thousands more. Interest in the vaccine was modest. Its creator, Maurice Hilleman, was never lionized as Salk had been.
“People felt, ‘What’s the big deal? I had measles; why does my kid need a vaccine?’ It was a very difficult sell,” said Walter Orenstein, an Emory University professor who headed the national immunization program at the Centers for Disease Control and Prevention from 1988 to 2004.
When a coronavirus vaccine becomes available, will it be met with a roaring ovation, like the polio vaccine, or communal yawning, like the measles shot? Or some strange hybrid of the two? Americans’ trust in authority, affordable access to the vaccine and a sense of solidarity will determine the result, said Orenstein and other public health veterans and historians.
Perceptions of particular diseases — and vaccines — reflect the seriousness of the diseases themselves, but popular values, culture, human risk assessment and politics all play important roles. Acceptance of public health measures — be they face masks or vaccines — is never entirely determined through a rational balancing of risk and benefit.
We can see that in the history of national campaigns for new vaccines meant to vanquish a scourge. No disease was more feared in the mid-20th century than polio. With the possible exception of AIDS, no disease since has been as feared until the arrival of COVID-19.
The polio vaccine was one of the few the public greeted eagerly. Diseases like measles and whooping cough were familiar childhood afflictions. In most years they killed more children than polio, but polio, which put people in iron lungs and leg braces, was visible in ways that an infant’s death certificate, tucked away in a drawer, could never be.
Vaccines are often a hard sell, since they prevent rather than cure disease and seem scary even though they are generally quite safe. Since vaccines must be widely used to prevent outbreaks, successful vaccination campaigns rely heavily on trust in those who sell, recommend and administer the medicines. And trust in science, government and business has not always been in steady supply.
In the late 1800s and early 1900s, when public health laws were in flux, authorities battling smallpox epidemics would often send vaccinators out with police to enforce the jab. They’d enter factories where cases had been reported, lock the doors and frog-march the workers through a vaccination line. The workers’ resistance was not unmerited; the vaccine sometimes caused swollen arms, fever and bacterial infections. Vaccination could cost a week’s missed wages.
Authorities had learned their lesson by the 1920s, when the diphtheria vaccine came on the scene, as James Colgrove notes in his book “State of Immunity: The Politics of Vaccination in Twentieth-Century America.” Diphtheria was a much-feared killer of children, and publicity campaigns run by public health officials, insurance companies and charities sought to educate and persuade rather than coerce.
Polio terrified Americans, peaking in 1952 with more than 57,000 cases. In 1938, President Franklin D. Roosevelt, himself a polio patient, had begun a national scientific program to battle the disease, backed by millions of Americans’ contributions through the March of Dimes.
The result of this national quest, uniting government and the people, was Jonas Salk’s inactivated polio vaccine. It cemented a powerful post-World War II trust in the U.S. scientific and medical establishment that would endure for many years.
Social solidarity was also important.
Vaccines prevent the circulation of a disease among the unvaccinated via what scientists call herd immunity — if enough people are vaccinated. When a reliable rubella vaccine became available in 1969, states quickly required childhood vaccination, even though rubella was practically harmless in children. They wanted to protect a vulnerable population — pregnant women — to prevent a repeat of the 1963-64 congenital rubella epidemic, which resulted in 30,000 fetal deaths and the birth of more than 20,000 babies with severe disabilities.
The embrace of the rubella vaccine, as historian Elena Conis of the University of California-Berkeley notes in her book, “Vaccine Nation: America’s Changing Relationship With Immunization,” marked the first time a vaccine had been deployed that offered no direct benefit to those who were vaccinated.
Still, it took a combination of fear, solidarity — and coercion — for Orenstein and his colleagues at the CDC and state public health agencies to drive childhood vaccination rates for measles, whooping cough, rubella and diphtheria to 90% and above in the 1990s to assure herd immunity.
Shame was also a tool. Orenstein remembered testifying to the Florida Legislature when it was considering a tougher vaccine mandate. He showed them that disease rates were lower in neighboring states that had tighter mandates. It worked.
What’s different now? In a politically divided nation, trust in science is low and experts are distrusted, politicians more so. Childhood vaccination efforts are already beset by large numbers of hesitant parents. And efforts to fight the COVID epidemic in the United States have been clumsy and chaotic at best, leaving Americans to doubt the competence of their governments and institutions.
There is still fear. “Maybe I’m an old-fashioned fool, but I think that most people will welcome a vaccine, if the rollout is done right,” said David Oshinsky, a professor of history at New York University and author of “Polio: An American Story,” a Pulitzer Prize-winning history. “Most people are desperately afraid of COVID. A minority thumb their noses, many of them for political reasons. How will this change when there’s a vaccine that [hopefully] changes the health risk equation to some degree?”
“A lot of people will be really eager to get it,” she said. “A lot will be hesitant, not only because of misinformation but because of a lack of trust in the current administration.”
When a coronavirus vaccine is introduced, it may be sold as personal protection, even for young, healthy people. But those who suffer most from the virus are usually older or sicker. An effective vaccination campaign may try to instill a sense of solidarity, or altruism, as well as a more general sense that without vaccination, the economy can’t get back on its feet.
“I’m not clear if people accept that solidarity,” Orenstein said. “People look more for what’s good for themselves than what’s good for society.” That said, the risk of COVID-19 to young people is “not zero. That’s one of the major ways to sell this, in a sense.”
MEDFORD, Ore. — From the outside, it appears to be just another suburban allergy clinic, a tidy, tan brick-and-cinder-block building set back from a busy highway and across the road from an auto parts store.
But inside the offices of the Clinical Research Institute of Southern Oregon, Dr. Edward Kerwin and his staff are part of the race to save the world.
Kerwin, 63, was tapped this spring to lead one of the nearly 90 U.S. clinical trial sites taking part in the large-scale, phase 3 test of a vaccine produced by biotech startup Moderna to fight the virus that causes COVID-19.
Starting in late July, Kerwin’s clinic, set in a working-class region roughly halfway between Seattle and San Francisco, began enrolling up to 40 participants a day for the two-year study. He hopes to recruit as many as 700 volunteers by the end of August.
They’ll join the 30,000 test subjects needed nationwide to determine whether the Moderna vaccine can tame a disease that has infected 5.4 million Americans and claimed the lives of more than 170,000. Another vaccine, produced by Pfizer and BioNTech, a German company, is being tested in nearly 30,000 more recruits.
“It’s a perfect opportunity for science to come to the rescue,” said Kerwin, a lanky figure in a bright-blue shirt and khaki pants. He led visitors to a conference room, took a chair well outside social-distancing range and doffed his mask, the better to explain the magnitude of this moment.
He acknowledged “it may seem like a surprise” that Medford is the site of a clinical trial to halt the world’s biggest medical challenge in a century. But Kerwin, who worked as a NASA scientist before heading to medical school and a career in allergy, asthma and immunology, has led more than 750 clinical trials over the past quarter-century, mostly focused on asthma, lung disease and skin disorders.
He moved to southern Oregon in 1993, choosing the rural Rogue Valley because of its beauty and cultural opportunities, such as the Oregon Shakespeare Festival in Ashland. As his medical expertise grew, he built a top-enrolling clinical trial site that coexists with a clinic that treats asthma and allergy patients. Along the way, he established deep roots in the valley, where he founded Bel Fiore, a $10 million winery and vineyard that features a 19,000-square-foot chateau.
Even with his experience, however, testing a vaccine to halt a global pandemic is a challenge like no other, Kerwin said. When the call came from Velocity Clinical Research — the North Carolina-based company that operates Kerwin’s clinic, known as CRISOR, and more than a dozen other COVID trial sites across the U.S. — he paused for a moment.
“You take a big gasp and say, ‘Do we have the resources to do this?’” Kerwin said. “You definitely do it, but you want to do your homework.”
So far, the testing is going well, he said. Unlike most clinical trials, for which it’s difficult to recruit enough volunteers, the COVID effort has attracted intense interest. All of Velocity’s sites are paying participants $1,962 for the two-year trial, but Kerwin’s staff of two dozen didn’t advertise widely at first.
“We would worry our phone would ring off the hook,” Kerwin said.
The Medford clinic is the only COVID vaccine clinical trial site in Oregon, so participants have come from as far as Portland, nearly 300 miles north.
It’s a prime example of the gamble drugmakers and federal trial sponsors take when deciding where to host large-scale COVID clinical trials. To gauge whether the vaccine works, you need to know there’s a good chance participants will be exposed to the virus in the environment. Ethically, in traditional phase 3 trials, you can’t deliberately infect people with COVID, a disease with no treatment or cure, though some propose doing just that in controversial human challenge trials.
Southern Oregon has not been a hot spot for COVID, with fewer than 500 confirmed cases and two deaths in Jackson County, which includes Medford. But, Kerwin said, it’s at risk of becoming one, offering the opportunity to vaccinate trial participants before the virus becomes widespread.
“It’s almost too late in New York and Arizona,” he said.
In the meantime, he’s trying to shift the odds that trial volunteers will be exposed to COVID-19 by reaching out to people at greater risk of infection.
So Kerwin’s team has contacted businesses in industries such as agriculture and food production, where the disease has been known to spread with particular virulence. Locally, that includes employers such as Harry & David, the food retailer famous for its fruit-of-the-month shipments, and Amy’s Kitchen, the maker of vegetarian frozen meals, which operates a production plant in the area.
The Medford trial site is also emphasizing enrollment of elder volunteers, those age 65 and up, who are at higher risk of serious illness or death from the coronavirus.
One of the first volunteers was Trish Malone, a 68-year-old cultural anthropologist who lives in Ashland. Like many of the other participants, she has enlisted in Kerwin’s previous clinical trials of devices to treat asthma. When clinic staffers reached out to ask whether she’d participate in the COVID trial, she didn’t hesitate.
“I said, ‘Wow, yes,’” Malone recalled. “It’s because of [Kerwin] and his expertise. Little Medford gets to have this testing.”
Participating is a way to “give back” to her community, said Malone, who sat, calm and still, on a recent Thursday as study coordinator Audrey Kuehl sank the injection into Malone’s left shoulder.
“She was fast. It was no pain, and it was fine,” Malone said.
Half of the patients in the trial will receive two doses, 28 days apart, of the Moderna vaccine, called mRNA-1273. It uses a snippet of the genetic code of the coronavirus, not the virus itself, to instruct cells to produce a protein that triggers an immune response to protect against infection. The other half will receive a placebo, or saline dummy shot.
Three study coordinators at the Medford clinic, Kuehl among them, know which patients receive which dose, but the information is kept from volunteers and other staff members — including Kerwin, the principal investigator.
Participants who receive the vaccine may experience some side effects, such as redness at the injection site, muscle soreness, fatigue or headache, Kerwin said. “It’s a sign the vaccine is working with your immune system,” he said.
Four days after her first injection, Malone was disappointed to report no reaction at all. “I am bummed, totally bummed,” she said. “I have no symptoms. I think I got the placebo.”
That may not be true, of course. Even if it is, Malone said, she’s happy to participate in an effort that may help stop the deadly virus.
“This a global pandemic,” she said. “What can I do to help?”
The study will run for two years so that investigators can track the longer-term effects of the vaccine. Malone will keep a diary of her temperature and symptoms, if any, and have regular blood tests to determine whether she has antibodies to the virus.
Kerwin is optimistic about the chances the Moderna vaccine will work, agreeing with Dr. Anthony Fauci, the nation’s top infectious disease expert, who predicted the study could demonstrate efficacy by November or December. Kerwin estimates that the vaccine could prove 90% effective, though outside infectious disease experts said it’s far too soon to tell.
Even if the trial shows the vaccine is successful, it would take months longer to produce and deliver enough injections for the U.S. and beyond.
As he enrolls patients and awaits data, Kerwin said, he’s mindful of the real-world implications of his work. His mother, in her 90s, lives in a Denver nursing home where, so far, there have been no cases of COVID-19. But the threat looms.
The tragedy of the pandemic has underscored the promise of science — and the interconnectedness of people far beyond this small corner of Oregon.
“Immunology has never been more fascinating than it is today,” he said. “This is a year that reminds us we cannot live in isolation and do not live in isolation from the world.”
Shortages of personal protective equipment and medical supplies could persist for years without strategic government intervention, officials from health care and manufacturing industries have predicted.
Officials said logistical challenges continue seven months after the coronavirus reached the United States, as the flu season approaches and as some state emergency management agencies prepare for a fall surge in COVID-19 cases.
Although the disarray is not as widespread as it was this spring, hospitals said rolling shortages of supplies range from specialized beds to disposable isolation gowns to thermometers.
“A few weeks ago, we were having a very difficult time getting the sanitary wipes. You just couldn’t get them,” said Dr. Bernard Klein, chief executive of Providence Holy Cross Medical Center in Mission Hills, California, near Los Angeles. “We actually had to manufacture our own.”
This same dynamic has played out across a number of critical supplies in his hospital. First masks, then isolation gowns and now a specialized bed that allows nurses to turn COVID-19 patients onto their bellies — equipment that helps workers with what can otherwise be a six-person job.
“We’ve seen whole families come to our hospital with COVID, and several members hospitalized at the same time,” said Klein. “It’s very, very sad.”
Testing supplies ran short as the predominantly Latino community served by Providence Holy Cross was hit hard by COVID, and even as nearby hospitals could process 15-minute tests.
“If we had a more coordinated response with a partnership between the medical field, the government and the private industry, it would help improve the supply chain to the areas that need it most,” Klein said.
Klein said he expected to deal with equipment and supply shortages throughout 2021, especially as flu season approaches.
“Most people focus on those N95 respirators,” said Carmela Coyle, CEO of the California Hospital Association, an industry group that represents more than 400 hospitals across one of America’s hardest-hit states.
She said she believed COVID-19-related supply challenges will persist through 2022.
“We have been challenged with shortages of isolation gowns, face shields, which you’re now starting to see in public places. Any one piece that’s in shortage or not available creates risk for patients and for health care workers,” said Coyle.
At the same time, trade associations representing manufacturers said persuading customers to shift to American suppliers had been difficult.
“I also have industry that’s working only at 10-20% capacity, who can make PPE in our own backyard, but have no orders,” said Kim Glas, CEO of the National Council of Textile Organizations, whose members make reusable cloth gowns.
Manufacturers in her organization have made “hundreds of millions of products,” but, without long-term government contracts, many are apprehensive to invest in the equipment needed to scale up the business and eventually lower prices.
“If there continues to be an upward trajectory of COVID-19 cases, not just in the U.S. but globally, you can see those supply chains breaking down again,” Glas said. “It is a health care security issue.”
For the past two decades, personal protective equipment was supplied to health care institutions in lean supply chains in the same way toilet paper was to grocery stores. Chains between major manufacturers and end users were so efficient, there was no need to stockpile goods.
But in March, the supply chain broke when major Asian PPE exporters embargoed materials or shut down just as demand increased exponentially. Thus, health care institutions were in much the same position as regular grocery shoppers, who were trying to buy great quantities of a product they never needed to stockpile before.
“I am very concerned about long-term PPE shortages for the foreseeable future,” said Dr. Susan Bailey, president of the American Medical Association.
“There’s no question the situation is better than it was a couple of months ago,” said Bailey. However, many health care organizations, including her own, have struggled to obtain PPE. Bailey practices at a 10-doctor allergy clinic and was met with a 10,000-mask minimum when they tried to order N95 respirators.
“We have not seen evidence of a long-term strategic plan for the manufacture, acquisition and distribution of PPE” from the government, said Bailey. “The supply chain needs to be strengthened dramatically, and we need less dependence on foreign goods to manufacture our own PPE in the U.S.”
Some products have now come back to be made in the U.S. — although factories are not expected to be able to reach demand until mid-2021.
“A lot has been done in the last six months,” said Rousse. “We are largely out of the hole, and we have planted the seeds to render the United States self-sufficient,” said Dave Rousse, president of the Association of the Nonwoven Fabrics Industry.
In 2019, 850 tons of the material used in disposable masks was made in the U.S. Around 10,000 tons is expected to be made in 2021, satisfying perhaps 80% of demand. But PPE is a suite of items — including gloves, gowns and face shields — not all of which have seen the same success.
“Thermometers are becoming a real issue,” said Cindy Juhas, chief strategy officer of CME, an American health care product distributor. “They’re expecting even a problem with needles and syringes for the amount of vaccines they have to make,” she said.
Federal government efforts to address the supply chain have foundered. The Federal Emergency Management Agency, in charge of the COVID-19 response, told congressional interviewers in June it had “no involvement” in distributing PPE to hot spots.
Project Airbridge, an initiative headed by Jared Kushner, President Donald Trump’s son-in-law, flew PPE from international suppliers to the U.S. at taxpayer expense but was phased out. And the government has not responded to the AMA’s calls for more distribution data.
Arguably, Klein is among the best placed to weather such disruptions. He is part of a 51-hospital chain with purchasing power, and among the institutions that distributors prioritize when selling supplies. But tribulations continue even in hospitals, as shortages have pushed buyers to look directly for manufacturers, often through a swamp of companies that have sprung up overnight.
Now distributors are being called upon not just by their traditional customers — hospitals and long-term care homes — but by nearly every segment of society. First responders, schools, clinics and even food businesses are all buying medical equipment now.
“There’s going to be lots of other shortages we haven’t even thought about,” said Juhas.
GARDENA, Calif. — Daisy Conant, 91, thrives off routine.
One of her favorites is reading the newspaper with her morning coffee. But, lately, the news surrounding the coronavirus pandemic has been more agitating than pleasurable. “We’re dropping like flies,” she said one recent morning, throwing her hands up.
“She gets fearful,” explained her grandson Erik Hayhurst, 27. “I sort of have to pull her back and walk her through the facts.”
Conant hasn’t been diagnosed with dementia, but her family has a history of Alzheimer’s. She had been living independently in her home of 60 years, but Hayhurst decided to move in with her in 2018 after she showed clear signs of memory loss and fell repeatedly.
For a while, Conant remained active, meeting up with friends and neighbors to walk around her neighborhood, attend church and visit the corner market. Hayhurst, a project management consultant, juggled caregiving with his job.
Then COVID-19 came, wrecking Conant’s routine and isolating her from friends and loved ones. Hayhurst has had to remake his life, too. He suddenly became his grandmother’s only caregiver — other family members can visit only from the lawn.
[khn_two_photos photo-first=”353172″ photo-second=”353180″ /]
After their walk, Daisy Conant and her grandson rest in front of their home in Gardena, California.
The coronavirus has upended the lives of dementia patients and their caregivers. Adult day care programs, memory cafes and support groups have shut down or moved online, providing less help for caregivers and less social and mental stimulation for patients. Fear of spreading the virus limits in-person visits from friends and family.
These changes have disrupted long-standing routines that millions of people with dementia rely on to help maintain health and happiness, making life harder on them and their caregivers.
[khn_slabs slabs=”241884″ view=”inline”]
“The pandemic has been devastating to older adults and their families when they are unable to see each other and provide practical and emotional support,” said Lynn Friss Feinberg, a senior strategic policy adviser at AARP Public Policy Institute.
Nearly 6 million Americans age 65 and older have Alzheimer’s disease, the most common type of dementia. An estimated 70% of them live in the community, primarily in traditional home settings, according to the Alzheimer’s Association 2020 Facts and Figures journal.
People with dementia, particularly those in the advanced stages of the disease, live in the moment, said Sandy Markwood, CEO of the National Association of Area Agencies on Aging. They may not understand why family members aren’t visiting or, when they do, don’t come into the house, she added.
“Visitation under the current restrictions, such as a drive-by or window visit, can actually result in more confusion,” Markwood said.
Daisy Conant and grandson Erik Hayhurst chat with a family friend on a Zoom call. Hayhurst is using Zoom to keep his grandmother connected to family and friends.
The burden of helping patients cope with these changes often falls on the more than 16 million people who provide unpaid care for people with Alzheimer’s or other dementias in the United States.
The Alzheimer’s Association’s 24-hour Helpline has seen a shift in the type of assistance requested during the pandemic. Callers need more emotional support, their situations are more complex, and there’s a greater “heaviness” to the calls, said Susan Howland, programs director for the Alzheimer’s Association California Southland Chapter.
“So many [callers] are seeking advice on how to address gaps in care,” said Beth Kallmyer, the association’s vice president of care and support. “Others are simply feeling overwhelmed and just need someone to reassure them.”
Because many activities that bolstered dementia patients and their caregivers have been canceled due to physical-distancing requirements, dementia and caregiver support organizations are expanding or trying other strategies, such as virtual wellness activities, check-in calls from nurses and online caregiver support groups. EngAGED, an online resource center for older adults, maintains a directory of innovative programs developed since the onset of the COVID-19 pandemic.
They include pen pal services and letter-writing campaigns, robotic pets and weekly online choir rehearsals.
Gina Moran helps her mother, who was diagnosed with Alzheimer’s in 2007, put on her mask. Gina Moran sometimes has trouble getting her mother to wear the mask.
Alba Moran must be reminded about the coronavirus pandemic when she is asked to wear her mask.
Hayhurst has experienced some rocky moments during the pandemic.
For instance, he said, it was hard for Conant to understand why she needed to wear a mask. Eventually, he made it part of the routine when they leave the house on daily walks, and Conant has even learned to put on her mask without prompting.
“At first it was a challenge,” Hayhurst said. “She knows it’s part of the ritual now.”
People with dementia can become agitated when being taught new things, said Dr. Lon Schneider, director of the Alzheimer’s Disease Research Center at the University of Southern California. To reduce distress, he said, caregivers should enforce mask-wearing only when necessary.
That was a lesson Gina Moran of Fountain Valley, California, learned early on. Moran, 43, cares for her 85-year-old mother, Alba Moran, who was diagnosed with Alzheimer’s in 2007.
“I try to use the same words every time,” Moran said. “I tell her there’s a virus going around that’s killing a lot of people, especially the elderly. And she’ll respond, ‘Oh, I’m at that age.’”
If Moran forgets to explain the need for a mask or social distancing, her mother gets combative. She raises her voice and refuses to listen to Moran, much like a child throwing a tantrum, Moran said. “I can’t go into more information than that because she won’t understand,” she said. “I try to keep it simple.”
The pandemic is also exacerbating feelings of isolation and loneliness, and not just for people with dementia, said Dr. Jin Hui Joo, associate professor of psychiatry and behavioral sciences at the Johns Hopkins University School of Medicine. “Caregivers are lonely, too.”
When stay-at-home orders first came down in March, Hayhurst’s grandmother repeatedly said she felt lonesome, he recalled. “The lack of interaction has made her feel far more isolated,” he said.
To keep her connected with family and friends, he regularly sets up Zoom calls.
But Conant struggles with the concept of seeing familiar faces through the computer screen. During a Zoom call on her birthday last month, Conant tried to cut pieces of cake for her guests.
Moran also feels isolated, in part because she’s getting less help from family. In addition to caring for her mom, Moran studies sociology online and is in the process of adopting 1-year-old Viviana.
Right now, to minimize her mother’s exposure to the virus, Moran’s sister is the only person who visits a couple of times a week.
“She stays with my mom and baby so I can get some sleep,” Moran said.
Before COVID, she used to get out more on her own. Losing that bit of free time makes her feel lonely and sad, she admitted.
“I would get my nails done, run errands by myself and go out on lunch dates with friends,” Moran said. “But not anymore.”
Gina Moran juggles several roles. She is the full-time caregiver to both her mother and baby, and studies sociology online.
The creator of the Polish website Agnostics and Atheists in AA recently asked me a number of questions. Here are the questions and my answers.
By Roger C
How long have you been in AA?
I’ve been in AA since I got sober a little over a decade ago (March 8, 2010). However, after three months of attending mainstream AA meetings, I became terrified that I would start drinking again, because I couldn’t stand the meetings. All the God stuff, you know. And the meetings ending with the Lord’s Prayer. I then accidentally discovered the oldest secular AA meeting in Canada, Beyond Belief Agnostics and Freethinkers, started in Toronto, Ontario on September 24, 2009. I went to the meeting. I loved the meeting! I remember walking along Bloor Street after it was over and I threw my hands up in the air and shouted “I’m saved!”
Are you an agnostic or an atheist?
I am an agnostic. Life to me is a “Magical Mystery Tour”, as per the Beatles. I certainly don’t believe in a anthropomorphic, interventionist, male deity. Not a chance. I should also note that I have a Master’s degree in Religious Studies obtained from McGill University in Montreal, Québec.
As an agnostic I studied and taught there for a decade, and I read the New Testament in its original language, Koine Greek. But I was always an agnostic. And everybody at McGill knew that and I was treated with great respect.
So, as an agnostic, what was I doing in the Faculty of Religious Studies? Well, one of my main reasons was to figure out why people believe in a supernatural, anthropomorphic deity. It is my understanding that it isn’t until we humans are about nine years old that we realize that our lives will end – with our death. Oh, my! So a main reason for religious belief is the denial of mortality and the invention of immortality – of course not for all other animals but just for we human animals.
Moreover and as a consequence religion is a cultural issue. As Richard Dawkins puts it in his book The God Delusion “Though the details differ across the world, no known culture lacks some version of the… anti-factual… fantasies of religion.” (p. 166). And that is passed along from one generation to another. Religion is hammered into children by their parents. It was certainly obvious that religion had been a key part of the early lives of the soon to be ordained ministers at McGill University.
Did you immediately reveal in the AA fellowship that God was not a part of your recovery?
Yes I did. And it was the huge disrespect I got at mainstream AA meetings as a result that really disturbed me, and made me want to get the hell out.
Is your home group a special group for agnostics and atheists, or is it a regular AA meeting?
I attended three secular AA meetings in Toronto – Beyond Belief Agnostic and Freethinkers, We Agnostics and We Are Not Saints – for roughly six years until I started the We Agnostics meeting in Hamilton (an hour away from Toronto) on Thursday, February 4, 2016. The meeting was a huge success and a second We Agnostics meeting on Mondays was launched on September 10, 2018. Of course since mid-March of this year both have been zoom meetings.
But now – hallelujah! – the Face to Face meetings at the First Unitarian Church are scheduled to recommence on Monday, August 24. We will, of course, play it safe. As Heather, one of the meeting organizers put it, “I think we should err on the side of extreme caution”. There will, of course, be masks, hand sanitizing, social distancing…
But f2f meetings are important, particularly for newcomers to AA.
How many agnostic AA groups are there in the area you live in?
In Hamilton there is only the one We Agnostics group, with two meetings. Toronto has some 500 AA meetings a week. Ten of the groups are secular and there is a secular AA meeting each and every day (when there is no pandemic). In all of the province of Ontario there are 20 secular AA groups and 24 meetings every week.
If an agnostic or an atheist asks you for sponsoring do you use the Big Book or do you rely on other texts?
No, I do not use the Big Book. The word “God” (or “He” or “Him” etc.) is used 281 times in the first 164 pages of the Big Book. A Christian God, by the way. The book is hugely disrespectful of non-believers and of women. I have published, via AA Agnostica, a total of eight secular AA books. One of them was written by two women back in 1991. It’s called The Alternative 12 Steps – A Secular Guide to Recovery. When I first found the book, it had been out of print for over a decade. In order to publish a second edition, I needed the permission of the authors, and it took me a year to find them. I published the second edition in 2014.
Today, another one of my favorite books is Staying Sober Without God. Published in 2019, it also has a good set of 12 steps called The Practical Steps.
What was the reason you started the AA Agnostica website?
Interesting question! The website was initially called “AA Toronto Agnostics” and was launched by another fellow and me in June of 2011 when the two secular AA groups in the city, including mine, Beyond Belief Agnostics and Freethinkers, were booted out of the Greater Toronto Area Intergroup (GTAI). And why were we booted out? Well, because we used a secular version of the 12 Steps. That resulted in a war that lasted for almost six years and was resolved in January 2017, when the groups were re-admitted to the GTAI as legitimate and respected members, with their secular 12 Steps.
Anyway, after six months I changed the name of the website to AA Agnostica. While initially its sole purpose was to provide information about the times and locations of the secular AA meetings it quickly became a popular site where atheists, agnostics and freethinkers in AA could share their views. Finally, a place where they could do that! That’s the historical significance of the website. Since then over 600 articles have been posted on AA Agnostica, usually one every Sunday and sometimes on Wednesdays.
How do you get articles for the website?
Click on the image for more information.
There are many ways. First, there is a widget on the home page of the AA Agnostica website that invites people to write an article. Even without that, a number of people who visit AA Agnostica are motivated to write an article. And I will from time to time invite various people – because of their comments, articles they have written elsewhere, etc. – to write for AA Agnostica.
Let me also add that I avoid negative articles, in particular those whose sole purpose is to attack mainstream Alcoholics Anonymous. While there are many problems with mainstream or traditional AA – and critiques are welcome! – mere grumbling and griping is not helpful.
What is your opinion about publishing brochures for agnostics in AA?
I think brochures are a good idea. When I started the We Agnostics meeting in Hamilton I created a brochure about the meeting and I brought it to every mainstream AA meeting – usually about a half hour before the meeting started – and asked them to put copies on their literature table. Some of them did and some of them threw the brochures out. But it was very helpful in terms of getting people to attend our meeting. And recently I posted an article on AA Agnostica about brochures/pamphlets encouraging people to create their own: Secular AA Pamphlets.
Have you thought about organizing annual workshops for agnostics and atheists in AA?
Two – not annual but biennial – workshops have already been organized for agnostics and atheists in AA in Ontario. We call them conferences or roundups. And the ones in Ontario are called SOAAR – Secular Ontario Alcoholics Anonymous Roundup. The first was held in Toronto in 2016. I was one of the organizers of the second SOAAR, held in Hamilton in 2018. (There are articles about both on AA Agnostica.)
At the one in Hamilton one on the speakers was Jeffrey Munn, the author of Staying Sober Without God. He came all the way up from California! The next SOAAR, to be organized largely by the Brown Baggers, originally scheduled for 2020, will now be held in 2022, as a result of the pandemic and so it doesn’t interfere with the International Conference of Secular AA (ICSAA) which will be held near Washington, DC, in the fall of 2021.
Would you like to say something about the situation of agnostics and atheists in AA? How do you see the near and further future?
Well, I think AA needs to grow up. It’s a bit silly to totally depend upon a book published over 80 years ago. That’s the “Conference-approved” nonsense. And it’s absolutely absurd to be ending meetings with the Lord’s Prayer and then pretending to be “spiritual, not religious”. More nonsense.
Roughly 20 years ago the growth of mainstream AA peaked, in spite of the growth of the population – and the growth in the number of alcoholics. But the growth of the secular movement within AA has been impressive. Twenty years ago there were 36 secular AA meetings worldwide. Thirty six! And now, today, there are approximately 550 secular AA meetings.
Our growth – including our regional roundups and the three International Conferences of Alcoholics Anonymous (ICSAAs) – has already had an impact on mainstream AA. So: let’s keep it up!
University of Wisconsin-Madison scientists have discovered that a majority of back-pain patients they tested who were taking opioid painkillers produced anti-opioid antibodies. These antibodies may contribute to some of the negative side effects of long-term opioid use.
For decades, meteorologists have named hurricanes and ranked them according to severity. Naming and categorizing heat waves too could increase public awareness of the extreme weather events and their dangers, contends a newly formed group that includes public health and climate experts. Developing such a system is one of the first priorities of the international coalition, called the Extreme Heat Resilience Alliance.
Hurricanes get attention because they cause obvious physical damage, says Jennifer Marlon, a climate scientist at Yale University who is not involved in the alliance. Heat waves, however, have less visible effects, since the primary damage is to human health.
Heat waves kill more people in the United States than any other weather-related disaster (SN: 4/3/18). Data from the National Weather Service show that from 1986 to 2019, there were 4,257 deaths as a result of heat. By comparison, there were fewer deaths by floods (2,907), tornadoes (2,203) or hurricanes (1,405) over the same period.
What’s more, climate change is amplifying the dangers of heat waves by increasing the likelihood of high temperature events worldwide. Heat waves linked to climate change include the powerful event that scorched Europe during June 2019 (SN: 7/2/19) and sweltering heat in Siberia during the first half of 2020 (SN: 7/15/20).
Some populations are particularly vulnerable to health problems as a result of high heat, including people over 65 and those with chronic medical conditions, such as neurodegenerative diseases and diabetes. Historical racial discrimination also places minority communities at disproportionately higher risk, says Aaron Bernstein, a pediatrician at Boston Children’s Hospital and a member of the new alliance. Due to housing policies, communities of color are more likely to live in urban areas, heat islands which lack the green spaces that help cool down neighborhoods (SN: 3/27/09).
Aaron Bernstein, a pediatrician at Boston Children’s Hospital, says giving heat waves names and severity rankings may help save lives.John Wilcox for Coverage, a BCBS of MA news service
Part of the naming and ranking process will involve defining exactly what a heat wave is. No single definition currently exists. The National Weather Service issues an excessive heat warning when the maximum heat index — which reflects how hot it feels by taking humidity into account — is forecasted to exceed about 41° Celsius (105° Fahrenheit) for at least two days and nighttime air temperatures stay above roughly 24° C (75° F). The World Meteorological Organization and World Health Organization more broadly describe heat waves as periods of excessively hot weather that cause health problems.
Without a universally accepted definition of a heat wave, “we don’t have a common understanding of the threat we face,” Bernstein says. He has been studying the health effects of global environmental changes for nearly 20 years and is interim director of the Center for Climate, Health and the Global Environment at the Harvard T.H. Chan School of Public Health.
Defined categories for heat waves could help local officials better prepare to address potential health problems in the face of rising temperatures. And naming and categorizing heat waves could increase public awareness of the health risks posed by these silent killers.
“Naming [heat waves] will make something invisible more visible,” says climate communicator Susan Joy Hassol of Climate Communication, a project of the Aspen Global Change Institute, a nonprofit organization based in Colorado that’s not part of the new alliance. “It also makes it more real and concrete, rather than abstract.”
The alliance is in ongoing conversations with the National Oceanic and Atmospheric Administration, the World Meteorological Organization and other institutions to develop a standard naming and ranking practice.
“People know when a hurricane’s coming,” Hassol says. “It’s been named and it’s been categorized, and they’re taking steps to prepare. And that’s what we need people to do with heat waves.”
For over a thousand years, the various prayers of the Catholic Holy Mass remained largely unaltered. Starting in the 1960s, though, the Catholic Church began implementing changes to make the Mass more modern. One such change occurred on November 27, 2011, when the church attempted to unify the world’s English-speaking Catholics by having them all use the same wording. The changes were slight; for instance, instead of responding to the priest’s “The Lord be with you” with “And also with you,” the response became: “And with your spirit.”
The seemingly small modification sparked an uproar so fierce that some leaders warned of a “ritual whiplash.”
The new wording has stayed intact, but that outsize reaction did not surprise ritual scholars. “The ritual reflects the sacred values of the group,” says Juliana Schroeder, a social psychologist at the University of California, Berkeley. “Those [ritual actions] are nonnegotiable.”
But in the midst of the global coronavirus pandemic, people are being forced to renegotiate rituals large and small. Cruelly, a pandemic that has taken more than half a million lives worldwide has disrupted cherished funeral and grieving rituals.
Even when rituals can be tweaked to fit the moment, such as virtual religious services or car parades in place of graduation ceremonies, the experiences don’t carry the same emotional heft as the real thing. That’s because the immutability of rituals — their fixed and often repetitive nature — is core to their definition, Schroeder and others say. So too is the symbolic meaning people attach to behaviors; doing the ritual “right” can matter more than the outcome.
Why do such behaviors even exist? Anthropologists, psychologists and neuroscientists have all weighed in, so much so that the theories used to explain the purpose of rituals feel as myriad as the forms rituals have taken the world over.
That growing body of research can help explain the unrest people are now experiencing as beloved rituals go virtual or get punted to some unsettled future. Multiple lines of evidence suggest, for instance, that rituals help with emotional regulation, particularly during periods of uncertainty, when control over events is not within reach. Rituals also foster social cohesion. Engaging in rituals, in other words, could really help people and societies navigate this new and fraught global landscape.
“This is exactly the time … when we want to be able to congregate with other people, get social support and engage in the kinds of collective rituals that promote cooperation [and] reduce anxiety,” says developmental psychologist Cristine Legare of the University of Texas at Austin. And yet, with COVID-19, congregating in any sort of group can be downright dangerous. What does that mean for how we persevere?
An illusion of control
Polish-born British anthropologist Bronislaw Malinowski documented rituals and speculated on their reason for being in the early 1900s. Living among fishermen on the Trobriand Islands off New Guinea from 1915 to 1918, Malinowski noticed that when the fishermen stuck to the safe and reliable lagoon, they described their successes and failures in terms of skill and knowledge.
But when venturing into deeper waters, the fishermen practiced rituals during all stages of the journey, acts Malinowski collectively referred to as “magic.” Before setting out, the men consumed special herbs and sacrificed pigs. While on the water, the fishermen beat the canoe with banana leaves, applied body paint, blew on conch shells and chanted in synchrony. Malinowski later used that Trobriand data to comment more broadly on human behavior.
“We find magic wherever the elements of chance and accident, and the emotional play between hope and fear, have a wide and extensive range. We do not find magic whenever the pursuit is certain, reliable and well under control of rational methods,” Malinowski wrote in an essay published posthumously in 1948.
Working in the late 1960s and early 1970s, American anthropologist Roy Rappaport built on that idea by developing a social framework for ritual, theorizing that such behaviors help individuals and groups maintain a balanced psychological state — much like a thermostat system that controls when the heat kicks on. In recent decades, anthropologists and psychologists have tested the idea that rituals regulate emotions.
In 2002, during a period of intense fighting between Palestine and Israel, anthropologist Richard Sosis took a taxi from Jerusalem to Tzfat, in northern Israel. Sosis, of the University of Connecticut in Storrs, noticed that the driver was carrying the Hebrew Bible’s Book of Psalms despite professing little religious inclination and admitting he didn’t read it. The driver said the book was there for his protection. Sosis suspected that the mere presence of the book helped the cabdriver manage the stress of possibly violent encounters. But how?
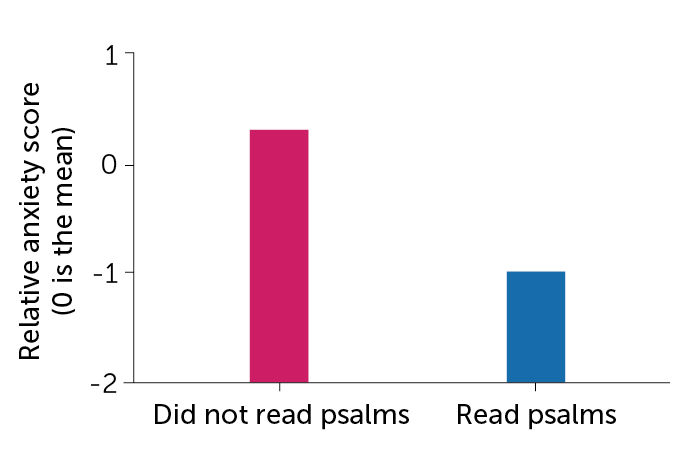
A few years later, Sosis and his team recruited 115 Orthodox Jewish women from Tzfat to take part in a study about psalm reading. By the time interviews began in August 2006, war between Israel and Lebanon’s Hezbollah had broken out; 71 percent of the women in the study had fled Tzfat for central Israel.
The researchers asked the women to list their three top stressors during the war. The women listed many of the same issues, with a few important differences. Almost 76 percent of those who stayed in Tzfat reported concerns about property damage compared with just 11 percent of women who left. Women who left were more likely than women who stayed to worry about stressors associated with displacement, such as inadequate child care (32 percent versus 9 percent) and a lack of schedule (32 percent compared with 6 percent).
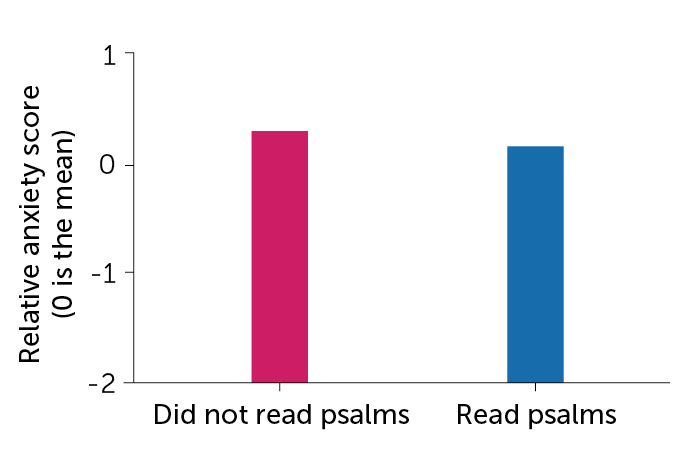
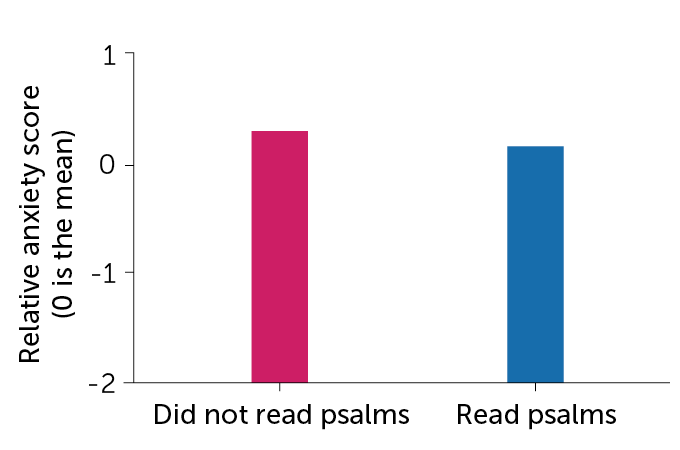
The researchers also had the women fill out a questionnaire about anxiety. Psalm reading provided anxiety relief, but the psalms’ true power depended on the women’s location. That is, the anxiety scores of women who left Tzfat and recited psalms were only slightly lower than the scores of women who left but did not recite psalms. The anxiety scores of women who stayed in Tzfat and recited psalms, on the other hand, were more than 50 percent lower than women who stayed and did not recite psalms. Overall, those who remained in Tzfat and recited psalms had lower anxiety scores than those who left.
When psalms help
Looking at psalm reading and anxiety levels among Orthodox Jewish women who stayed or fled war-torn Tzfat, Israel, in 2006, researchers found that anxiety scores were similar among women who read sacred texts and nonreaders who left, and nonreaders who stayed. But the anxiety levels of women in the war zone who read psalms were much lower than the other groups’.
Psalm reading helps when circumstances seem out of control
Left Tzfat
C. Chang
Remained in Tzfat
C. Chang
Source: R. Sosis and W.P. Handwerker/Am. Anthropologist 2011
“Reciting the psalms was effective under conditions in which the stressor was uncontrollable. But once you could devise instrumental solutions to a problem, such as taking care of your kids or finding work, reciting psalms isn’t going to fix anything,” says Sosis, whose findings appeared in American Anthropologist in 2011. Several more recent studies conducted on individuals living in war and earthquake zones mirror Sosis’ finding that rituals give participants a sense — or a comforting illusion — of control over the uncontrollable.
Testing the illusion
In recent years, researchers have begun testing the psychological benefits of rituals using controlled experiments and physiological monitors. In one study, Dimitris Xygalatas, an anthropologist and psychologist also at the University of Connecticut, and colleagues recruited 74 Hindu women in southwest Mauritius. Thirty-two women were sent to a lab and the rest to the local temple. All participants completed a survey evaluating their overall anxiety and were fitted with heart rate monitors.
Researchers elicited anxiety among the women by giving them three minutes to put together a speech on their flood preparedness — natural disasters are a common threat to the island — to ostensibly be evaluated later by government experts.
Afterward, women at the temple performed their usual routine — praying to Hindu deities and offering fruits and flowers. These actions tended to follow the same pattern across participants, such as holding an oil lamp or incense stick and moving it slowly clockwise before the statue of a deity. Women at the lab, meanwhile, sat quietly for 11 minutes, about the same time it took for the other women to pray. All participants then took a second anxiety survey.
D. XygalatasIn Mauritius, many women regularly pay tribute to the gods in the Hindu pantheon, such as this woman making an offering to Lakshmi, the goddess of wealth.
On the first survey, both groups reported similar levels of anxiety. But the women who then performed their rituals at the temple reported half as much anxiety as the women in the lab.
That divergence also showed up on the heart monitors, specifically on a marker for resilience known as heart rate variability. During periods of stress, heart rate becomes less variable and the time between beats gets shorter.
Spacing between heartbeats for women who sat quietly increased only about 3 percent from the baseline rate, measured when the women first arrived at the lab. But for women who performed the ritual and experienced stress reduction, the space between beats lengthened 22 percent from the baseline rate, Xygalatas and colleagues reported in the Aug. 17 Philosophical Transactions of the Royal Society B. That is, heart rate variability was 30 percent higher among women performing the ritual than women who sat quietly.
Worshippers in Mauritius hold trays bearing fruits and flowers as gifts to gods in the Hindu pantheon. D. Xygalatas
Xygalatas’ and Sosis’ studies suggest that engaging in the individual, repetitive rituals often seen in religious practices, such as reading psalms or reciting prayers, could serve as a balm during the pandemic. But, typically, even individual rituals carry a social component. For instance, it was common for women in Sosis’ study to divvy up the 150 passages so that they could read the entire Book of Psalms in a single day. “Women recognize that other women are also engaging in these psalm-recitation activities,” Sosis says.
Researchers largely concur that the power of rituals rests within a larger social fabric. Rituals “are created by groups, and individuals inherit them,” Legare says. The problem is, during the pandemic, even if people are engaging in rituals on their own, those larger groups are now fractured.
Merging with the in-group
The idea that rituals serve to bond individuals is not new. Fourteenth century scholar Ibn Khaldūn used the term asabiyah, Arabic for solidarity, to describe the social cohesion that emerges from engaging in collective rituals. Khaldūn believed that solidarity had its foundations in kinship but extended to tribes and even nations. Centuries later, in the early 1900s, French sociologist Émile Durkheim theorized that group rituals fostered unity among practitioners.
In contemporary times, researchers have sought to understand the ways in which rituals bind people together. Work by University of Oxford anthropologist Harvey Whitehouse suggests that rituals exist on either side of a dichotomy. On one side are “imagistic” rituals that fuse people together, often more tightly than kin, through intense moments and painful rites of passage, such as piercing or tattooing one’s body and walking on fire.
Today, imagistic rituals are much less common than the “doctrinal” rituals that characterize modern-day life — prayers, religious services and various regimented rites of passage, such as baby showers and birthday parties. Such rituals appear to have become established as societies grew increasingly complex with the emergence of agriculture. While not binding people as tightly as imagistic rituals, doctrinal rituals enable group members to both identify those in their larger group and spot and police social deviants, Whitehouse says.
Several studies of contemporary communities support the idea that doctrinal rituals help unite social groups. In the early 2000s, Sosis compared cooperation among members of secular versus religious collective farming settlements, called kibbutzim, in Israel. The two types of kibbutzim operated in similar ways, except that men in the religious settlements were required to pray in groups of 10 or more people at least three times a day. Women also prayed, but did not have to do so collectively. Sosis reported in Current Anthropology in 2003 that members of religious kibbutzim were more cooperative, as evidenced by taking less money out of a communal pot, than members of secular kibbutzim. That difference was driven entirely by those ritual-practicing men in the religious kibbutzim.
In her research, Legare — who invents rituals to see how children understand such practices — has shown that children use rituals to identify and reinforce connections with members of their own group while shunning those outside the group. Recently, Legare, working with Nicole Wen, now at Brunel University London, divided 60 children, ages 4 to 11, into two groups. The children were given wristbands denoting their group’s color. One group was then walked through a highly scripted, ritualized process to make a bead necklace with prompts like: “First, hold up a green string. Then, touch a green star to your head. Then, string on a green star” and so on. The other group made necklaces with the same materials, but no script.
The activities continued for two weeks, during which the researchers measured how long children spent comparing their handiwork to that of members of their own group and how long they spent watching members of the other group, such as by looking over their shoulders. Reporting in the Aug. 17 Philosophical Transactions of the Royal Society B, the team found that during the experiment, children in the ritual group spent on average twice as much time as children in the nonritual group showing off their necklaces to members of their own group and monitoring the behavior of those not in the group.
2X
Extra time that children who beaded necklaces using rituals, compared with children who beaded necklaces without ritual, spent showing off their handiwork and checking out the work of the other group
Working in a group helps people bond even without a script to follow, Legare says. But “rituals take the effects of a group experience and turn them way up.”
Legare’s project and others also illustrate how rituals engender in-groups and out-groups. Whitehouse’s work suggests that shared traumatic experiences, which may include imagistic rituals, contribute to the cohesion of terrorist cell networks, where fighters would sooner die for fellow fighters than even family (SN: 7/9/16, p. 18).
The pandemic itself is the latest example of how a shared traumatic experience and the resulting rituals — Zoom parties, alliances around wearing or eschewing masks and reactions to civil rights rallies — can break or bind communities.
“Human social groups … [are] always going to be vulnerable to in-group preferences and out-group biases,” Legare says. Whether we use ritual for good — or evil — is up to us.
Pandemic asynchrony
Certain rituals, such as singing and dancing together, are particularly good at amplifying group cohesion and a spirit of generosity. But these group rituals, tragically, also can spread the coronavirus.
On March 10 in Skagit County, Wash., 61 members of a church choir met for practice. One singer, who had been feeling unwell for a few days, later tested positive for COVID-19. Within weeks, almost 90 percent of those in attendance had developed similar symptoms, with 33 confirmed cases; two members died from the disease. Similar stories linking choir practice to superspreading events have emerged. And the collective singing that characterizes so many religious services has emerged as a particularly risky activity in this pandemic.
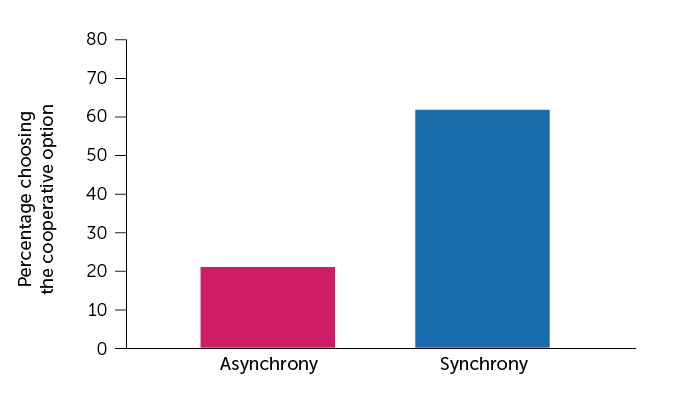
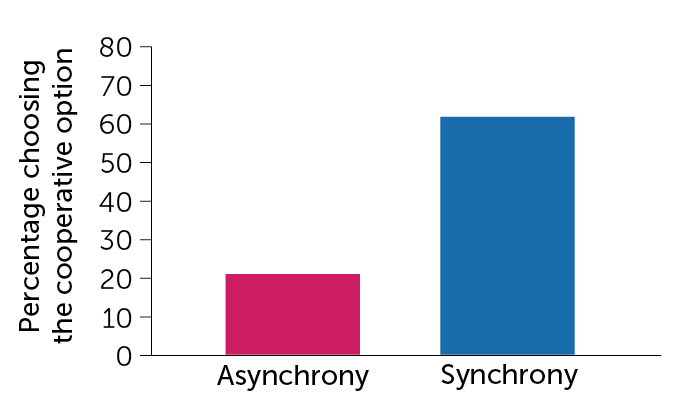
In a series of experiments reported in 2013, researchers tested to see if dancing or chanting together made people feel more generous toward members of their group. One of the tests divided 27 volunteers into groups of three and handed them a list of one-syllable words divided into three columns. The researchers told some of the groups to go down the list and chant the words together for six minutes, keeping in beat with a metronome — effectively a ritual performed in synchrony. Other groups recited the words sequentially, with each member reading the words in only one column.
The participants then played a cooperative game within their groups. Anonymously, each member could choose either option X, a guaranteed prize of $7, or option Y, a prize of $10 that came through only if every group member chose Y. If a single member chose X, no one would get money. Reporting in PLOS ONE, the researchers found that 62 percent of participants who chanted together chose Y compared with just 21 percent who chanted in sequence.
One for all
Participants who chanted as a group at the same time were more cooperative when playing a game after the chanting than those who chanted words sequentially.
Synchronous chanting increases cooperation
C. Chang
C. Chang
Source: P. Reddish et al/PLOS ONE 2013
Other synchronized activities, such as marching, dancing, rowing and even collective social distancing while out in public, can bond participants, Whitehouse says. The alliance forged by synchrony is arguably playing out across the United States even now as both Black and non-Black people march and chant in unison to protest police brutality and systemic racism. In any context, Legare says, synchrony “is a powerful social catalyst.”
New rituals
Ironically, as the pandemic makes practicing rituals, particularly social rituals, profoundly challenging, decades of research have made clear that people turn to such regimented behaviors during periods of unrest. “Anthropologists have long observed that during times of anxiety, you see spikes in ritual activity,” Xygalatas says.
So even as rituals are being disrupted and diluted, people are seeking new sources of solace. Many people, for instance, are turning to their immediate family members to fill that ritual void.
“It’s possible that lockdowns are actually leading to the invention of new family rituals that foster this kind of resilience, ranging from the arrangement of rainbows and teddy bears in windows to the revival of more traditional family rituals like eating, singing [and] telling stories together,” Whitehouse says.
People are also finding new ways to experience old traditions. Rachel Fraumann, a Methodist minister in Barre, Vt., says online attendance at her recorded sermons has more than doubled since mid-March. In her view, now is a great time for the ritually and spiritually adrift to shop around for their ritual fit.
Such “shopping” doesn’t need to occur within a religious context. Secular rituals, such as those centered around crafts, music or sports, have shown similar promises, and pitfalls, as religious activities, says Oxford cognitive anthropologist Martha Newson. Which means now could be a great time to try new hobbies with a solo component as a way to practice in the here and now, with a group component to look forward to after the pandemic ends, such as knitting with the goal of joining a knitting circle or buying a rowing machine to get fit enough to join the local crew team, where bodies move in sync.
Creating rituals outside of religion, though, can be hard to get right. “It’s not the hobby, it’s the people who do the hobby who make the tribe. Precisely what the magic ingredients are for that, we [don’t] know,” Newson says.
Those challenges won’t stop people from trying once the pandemic ends, Legare says. “I would predict that there will be an increase in attending religious services but [also] an increase in attending all kinds of social group activities. People are so starved for social interaction, I would predict increased enrollment in absolutely everything.”
 I am an agnostic. Life to me is a “Magical Mystery Tour”, as per the Beatles. I certainly don’t believe in a anthropomorphic, interventionist, male deity. Not a chance. I should also note that I have a Master’s degree in Religious Studies obtained from McGill University in Montreal, Québec.
I am an agnostic. Life to me is a “Magical Mystery Tour”, as per the Beatles. I certainly don’t believe in a anthropomorphic, interventionist, male deity. Not a chance. I should also note that I have a Master’s degree in Religious Studies obtained from McGill University in Montreal, Québec. No, I do not use the Big Book. The word “God” (or “He” or “Him” etc.) is used 281 times in the first 164 pages of the Big Book. A Christian God, by the way. The book is hugely disrespectful of non-believers and of women. I have published, via AA Agnostica, a total of eight secular AA books. One of them was written by two women back in 1991. It’s called The Alternative 12 Steps – A Secular Guide to Recovery. When I first found the book, it had been out of print for over a decade. In order to publish a second edition, I needed the permission of the authors, and it took me a year to find them. I published the second edition in 2014.
No, I do not use the Big Book. The word “God” (or “He” or “Him” etc.) is used 281 times in the first 164 pages of the Big Book. A Christian God, by the way. The book is hugely disrespectful of non-believers and of women. I have published, via AA Agnostica, a total of eight secular AA books. One of them was written by two women back in 1991. It’s called The Alternative 12 Steps – A Secular Guide to Recovery. When I first found the book, it had been out of print for over a decade. In order to publish a second edition, I needed the permission of the authors, and it took me a year to find them. I published the second edition in 2014.