August 29, 2020 – As he did at last year’s inaugural event, Father Neal Longe of St. Ann’s Episcopal Church will lead the crowd in prayer, while candles will be provided by Betz, Rossi & Bellinger Funeral Home and both signs and stickers will be provided by Sticker Mule.
“We’re looking forward to educating individuals about the stigma [of addiction],” Hill said. “It could be my family, it could be yours. It could be a neighbor, it could be a parent’s neighbor. It could be anyone, at any time, anywhere.” “It’s great that we do this every year,” she added, “but this something that we should be doing daily.”
According to the state Department of Health’s most recent County Opioid Quarterly Report issued in January, there were nine opioid overdose deaths in Montgomery County in 2018, and two from January through June 2019.
Montgomery County launched a task force last year to combat the opioid epidemic, as between 2015 to 2017 the county had the highest opioid prescription rate in the state, according to the Department of Health.
Combating the negative stigma of addiction is one key step to addressing the problem, Hill said, as is increasing the availability of and training for the use of Narcan (naxolone), the nasal spray that can be used to treat decreased breathing during an opioid overdose.
In the United States, the average wait time for COVID-19 test results is about four days. Even worse, 10 percent of individuals don’t receive lab results for 10 days or more.
Quick reporting of test results helps identify infected individuals so they and anyone they potentially spread the coronavirus to can be isolated, preventing further spread of the virus.
“If you have a 14-day lag to knowing if someone is actually sick and contagious, then they’ll interact with many, many more people in that period than if you have a one-day or a six-hour or one-hour turnaround,” says Omar Abudayyeh, a bioengineer at MIT.
Abudayyeh is among the many researchers and companies racing to develop new and speedier types of diagnostic tests that circumvent clinical labs altogether. Some of these tests complete their analyses in all-in-one machines that are portable enough to be set up in schools, nursing homes and offices. Several companies are developing tests like these that can diagnose COVID-19 in 30 minutes or less, with a level of accuracy comparable to lab tests. Others are harnessing the power of the gene editor CRISPR to deliver rapid results.
And another type of test, made by Abbott Laboratories and granted emergency use authorization by the U.S. Food and Drug Administration on August 26, works more like a pregnancy test. All it requires is a test card the size of a credit card, a few drops of a reaction solution and a sample from a nasal swab. Within 15 minutes, two lines appear on the card if the sample contains the virus; one line appears if it doesn’t.
The gold standard
The current gold standard for accurate COVID-19 testing is PCR, or polymerase chain reaction, which can detect even tiny quantities of the virus’s genetic material, RNA (SN: 3/6/20).
The test requires collecting viral RNA directly from the patient, typically gathered using a swab inserted deep into the nasal cavity. At a clinical laboratory, the virus’s RNA is converted to DNA and then run through a specialized instrument that heats and cools that DNA to multiply copies of it, making it easier to detect. After repeating the process for around an hour, if DNA shows up, the sample is considered positive for SARS-CoV-2, the virus that causes COVID-19.
Such tests are fairly accurate. They miss some people very early in the infection or because of lab errors, producing false negatives, meaning that the test results indicate someone isn’t infected when they really are. False positives — when tests wrongly indicate an uninfected person has the virus — are rare with this type of technology. So if a PCR test indicates a person is infected, they probably do carry the virus. The main drawback is the speed. It typically takes days to get results back, and backups at labs can drag the process out for a week or two.
Some people find the nasal probe uncomfortable, so other lab tests have been developed that rely on less invasive samples. On August 15, the FDA authorized a saliva-based test, SalivaDirect, for emergency use. This isn’t the first test to detect the SARS-CoV-2 virus in saliva, which is easier to collect than samples from nasal passages. But its simplified protocol speeds up sample preparation and bypasses testing supplies that have been in short supply in recent months. SalivaDirect, however, is not a rapid test. It still requires processing by clinical laboratories, which contributes to the wait time between providing a sample and receiving results.
To develop faster tests, companies are taking a variety of approaches. Funding for some of this work comes from the Rapid Acceleration of Diagnostics initiative, or RADx, from the National Institutes of Health, which has invested $248.7 million in seven companies tackling testing challenges.
Compact instruments, such as Mesa Biotech’s Accula test, replace the function of clinical labs and could bring rapid testing to schools, nursing homes and offices.Mesa Biotech
San Diego–based Mesa Biotech, for instance, received RADx funding to manufacture a PCR test that replaces an entire clinical lab with a handheld dock and a single-use cartridge. The company says the proprietary technology in its Accula test, which has already received FDA emergency use authorization, can provide a COVID-19 diagnosis in just 30 minutes.
Turning on the LAMP
Other RADx-funded companies, such as Talis Biomedical, headquartered in Menlo Park, Calif., aren’t using PCR to amplify SARS-CoV-2 viral material. The Talis One system instead uses LAMP, or loop-mediated isothermal amplification. In a typical LAMP assay, a patient’s nasal or oral swab sample is mixed with enzymes and specially designed DNA fragments, then heated to 65° Celsius to copy the viral RNA to DNA and produce many more DNA copies. With the Talis test, samples are placed in a cassette, popped into a specialized dock, and analyzed in just 30 minutes.
As opposed to an instrument that cycles between hot and cold, LAMP heats the reaction to one temperature. “You could run the reaction in a water bath,” says Nathan Tanner, a molecular biologist at New England Biolabs in Ipswich, Mass.
In general, LAMP-based diagnostic tests aren’t quite as sensitive as ones based on PCR, Tanner says, but could be used to test more people, given their simpler requirements. In one newly described LAMP testing method, a solution changes color in the presence of 100 or more SARS-CoV-2 RNA molecules. The authors, who describe the test August 12 in Science Translational Medicine, propose that the approach, which didn’t detect the lowest viral loads, would be suitable for identifying individuals with a moderate to high viral load.
Telltale proteins
A third RADx-funded test provides results in a mere 15 minutes. Rather than detecting viral RNA, the test, by Quidel, based in San Diego, detects proteins from virus particles. These viral proteins are also antigens, meaning they stimulate immune responses when they invade our bodies. Such antigen tests are similar to ones used in doctors’ offices and pharmacies to diagnose people with influenza.
Don’t confuse antigen tests with an antibody test that detects antibodies a person develops in response to an infection (SN: 4/28/20) Much like a pregnancy test, COVID-19 antigen tests use antibodies to detect the viral proteins and give a yes or no answer, says Kim Hamad-Schifferli, a bioengineer at the University of Massachusetts Boston.
The Quidel Sofia SARS antigen test has been authorized for emergency use. Like the other RADx-funded rapid tests, it uses a dock and single-use cartridges: Instead of making a line on stick the way a pregnancy test does, the dock detects a fluorescent signal if SARS-CoV-2 proteins are present.
An antigen test by Abbott Laboratories requires only a test card, a swab sample and a few drops of a reaction solution to return a COVID-19 diagnosis in 15 minutes.Abbott
Abbott Laboratories’ test granted emergency use authorization August 26 also is an antigen test and, with its card-based technology, is even simpler. Abbott, based in Abbott Park, Ill., said its test was able to detect 34 of 35 COVID-19-positive patients with symptoms, or 97 percent, in initial studies.
The benefit: An antigen test doesn’t require any specialized lab instruments or enzymes. “It’s all self-contained,” Hamad-Schifferli says. Without a step to amplify viral material, however, an antigen test can be less sensitive than PCR or LAMP and result in a higher rate of false-negative results, up to 20 percent per the FDA’s emergency use authorization guidelines for antigen tests.
That’s because people may produce widely varying amounts of virus, depending on how long has passed since they became infected. In most people, the coronavirus is most abundant from a couple of days after infection to about nine days into the illness (SN: 3/13/20). After that, the immune system kicks in, preventing viruses from being made. On the other hand, viral RNA can be detectable in some people for more than a month. A negative result from an antigen test has a higher chance of being false comfort, so the FDA says that diagnosis may need to be confirmed with another type of test, like PCR.
A new kind of rapid test
Even though antigen tests typically are not as accurate as standard PCR or the new rapid tests, they could play a crucial role helping to end the pandemic — if their use becomes widespread. As of now, though, even Abbott’s 15-minute test still needs to be ordered by a doctor and performed in a health care setting, so that can provide hurdles to its use. But what if people didn’t even have to leave home to get a test?
That’s what Hamad-Schifferli and her colleagues are working on. The idea is to build a cheaper test that doesn’t involve a dedicated instrument — just a paper strip and a signal detectable by eye. Such a simple test could be used more widely by people at home. “It would be a game changer,” she says.
If COVID-19 tests are deployed widely enough, they could serve as a public health measure to identify people with high levels of SARS-CoV-2 and spreading the virus to others, even if they’re not displaying symptoms. That’s because frequent and fast tests can be used to pinpoint outbreaks as they are happening (SN: 7/1/20). If cheap enough, these tests could be used by people daily, catching any missed detections through repeated rounds of testing.
But for daily, population-wide testing that could alert people when they first start transmitting the coronavirus to be adopted, a test needs to be cheap enough — for instance, under a dollar — for many people to use them frequently. Abbott said its tests would cost $5. Quidel’s test cartridges cost $23 apiece and the other RADx-funded rapid tests are likely in a similar price range. Given their higher accuracy, those tests could serve a separate purpose: to conclusively determine if an individual is infected and ensure they receive treatment.
With overwhelming demand for COVID-19 testing, it can take days or even longer than a week for people to receive test results.Hoptocopter/E+/Getty Images
The holy grail of tests may be one that is fast, easy, accurate and inexpensive and that could be used broadly — even by people at home. One group of scientists may be among those nearing that goal. The work is led by Abudayyeh, Jonathan Gootenberg and Feng Zhang, all bioengineers at the McGovern Institute for Brain Research at MIT. Zhang is also at the Broad Institute of MIT and Harvard University.
The team adapted an FDA-authorized test by Sherlock Biosciences in Cambridge, Mass., that uses the gene-editing tool CRISPR. All someone has to do is add a sample — either from a nasal swab or saliva — to a tube with a reaction solution, heat the tube to 60° C for an hour in a pot of water, then add a paper test strip to the tube. If two lines appear, that means SARS-CoV-2 RNA is present.
The readout relies on activity of a CRISPR enzyme, Cas12b. If SARS-CoV-2 RNA is present in the reaction, Cas12b cuts what’s called a reporter, a short piece of DNA that’s labeled on both ends. The two halves of the reporter then wick up the paper strip to different places and appear as two lines. If viral RNA isn’t present, the reporter remains intact and wicks up the strip to one place, showing up as one line.
The new test, STOPCovid, is not yet authorized for clinical use, but based on tests in a small number of patients, it identifies SARS-CoV-2 cases as well as PCR tests, the researchers reported May 8 in a preprint posted at medRxiv.org. It returns results in about an hour and would cost under $10, they say.
Unlike rapid tests relying on docks and cartridges, the STOPCovid test is uniquely designed to scale up to millions of tests per week, says Gootenberg. “There’s never been a demand for millions or tens of millions of tests per week — ever.”
With the development of so many new technologies to test for the coronavirus, “we’re going to come away from the epidemic with a whole new field of diagnostics,” Mina says.
As a veteran who served back-to-back tours in Iraq, I initially cringed when commentators compared the COVID-19 crisis to wartime — no bullets, no blood and no one volunteered for this.
But after my months of reporting on the pandemic, it has become painfully clear this is like war. People are dying every day as a result of government decisions — and indecision — and the death toll is climbing with no end in sight.
Less than six months into the pandemic, COVID-19 has already killed at least 183,000 Americans, more than triple the number who died in the Vietnam War, and far more than the wars in Iraq and Afghanistan combined.
We are all being asked to make sacrifices for the good of our country. And we’re experiencing, as a nation, a deeply traumatic event. Like war, the toll will be felt for a long time.
In California, local public health officials are leading the front lines in this battle against COVID-19, dictating strategy, issuing orders and developing tactics to carry out that strategy. Every day, they make gut-wrenching calls to protect our health and livelihoods, even if those decisions may inflict initial harm on the economy or contradict politicians and popular opinion.
But instead of being celebrated for their difficult and dangerous work, as I was, they are now facing violent threats and political attacks from those who disagree with their tactics — such as requiring masks in public and ordering businesses and parks closed to prevent the spread of infection.
When I interview them, often late at night, I hear in their voices that familiar mix of emotions that often come with war: exhaustion, anxiety and devotion to duty.
“We’ve become easy scapegoats for people’s fear and anxiety during COVID-19,” said Dr. Gail Newel, the health officer for Santa Cruz County, who continues to face threats for issuing public health orders.
The latest — a menacing email sent to her in late July calling her a “communist bitch” — prompted local law enforcement to recommend she get a guard dog and firearm to protect herself. “That weighs very heavily,” she said.
I can’t imagine the burden. Although many of us serving in Iraq disagreed with the war, we remained dedicated to our mission and enjoyed broad support at home.
I joined the military as a U.S. Army reservist in 1999 and was deployed on active duty to Iraq in early 2003, when it truly was like the Wild West.
Serving first as logistics clerk and then the acting supply sergeant for a military police company out of San Jose, California, I helped ensure my military brothers and sisters had proper equipment. When the George W. Bush administration sent us to Iraq, for example, it did so without armoring our Humvees — a major failure that elevated our risk of being blown up by roadside explosives.
I returned home in July 2004 and spent years putting the battlefield behind me as I transitioned to a career in journalism. But living through COVID-19 has resurrected those feelings of being at war.
Now, just like then, there is an overall sense of fear and uncertainty because we don’t know when the crisis will end. We aren’t free to go about our lives as we once did and we yearn for the comforts we took for granted. We miss our loved ones we can’t see.
We must remain hyper-vigilant to potential threats, and even make sure to don our “armor” when we leave our homes, except now it’s masks and gloves instead of helmets and flak jackets.
There’s something that happens when you’re in a conflict zone — the air feels heavier. You can feel threats all around you, just waiting to strike. There’s deep anxiety for what the future holds, and you wonder whether you’ll be alive next week or next month.
Public health officers are shouldering the added anxiety that duty brings. For much of the pandemic, Gov. Gavin Newsom has pushed the responsibility — and blame — of reopening largely onto counties and the state’s 61 local health officers, who have worked for months without days off, giving up time with their families to attack this crisis head-on.
I have interviewed dozens of them. Some have broken into tears while talking with me, and worry chokes their voices as they lament problems with testing or explain how they don’t have enough supplies or contact tracers to safely reopen. They felt rushed into lifting stay-at-home restrictions in May and June, yet they had no choice in the face of pressure from politicians and suffering residents and businesses. After years of severe underfunding, public health agencies don’t have the money or resources to deploy an adequate response.
They’re also wrestling with the guilt and trauma that come with making decisions that affect people’s lives and livelihoods.
“It has been hard on all of us,” acknowledged Sacramento County’s health officer, Dr. Olivia Kasirye. “We’re getting phone calls daily from people saying they’re going bankrupt and they can’t pay their rent and they have loved ones who are dying that they can’t see.”
I know how that feels, having been conflicted about our long-term strategy in the Middle East and the harm we inadvertently inflicted on innocent civilians. But I can’t imagine being afraid of the people I signed up to protect.
Public health officials have become targets of aggressive and personal attacks. Some have seen their photos smeared with Hitler mustaches, while others have had their personal phone numbers and home addresses circulated publicly, prompting the need for round-the-clock security.
“Imagine treating American soldiers and military families with the kind of hatred and disrespect that local health officers are facing,” said Dr. Charity Dean, unprompted, a day after she left her job as one of the top public health officials in the Newsom administration. “They’re the ones taking all the risk, and it makes me angry to see how they’ve been treated.”
Mimi Hall, Newel’s boss and Santa Cruz County’s top public health official, told me law enforcement is investigating a threatening letter addressed to her that was allegedly signed by a far-right anti-government extremist group.
In response, Hall considered retiring early. But she didn’t want to abandon her troops and wasn’t going to let fear stop her from doing her job. So she had a perimeter fence and home security system installed over the weekend — and reported for work promptly Monday morning.
Yes, we are waging a life-or-death battle in which innocent people are hurt, but it’s these battle-scarred public health officers who are making deeply personal sacrifices to steer us to safety.
We commemorate military leaders with medals and parades. Why not treat our public health officials with the same level of appreciation?
As you drift into unconsciousness before a surgery, general anesthetic drugs flowing through your blood are putting you to sleep by binding mainly to a protein in the brain called the ɣ-aminobutyric acid type A (GABAA) receptor. Now UT Southwestern scientists have shown exactly how anesthetics attach to the GABAA receptor and alter its three-dimensional structure, and how the brain can tell the difference between anesthetics and the psychoactive drugs known as benzodiazepines – which also bind to the GABAA receptor. The findings were published online today in the journal Nature.
I grew up as a Jehovah’s Witness and stayed until I was almost 30, about the time I started on my recovery path. I was a good little boy and young adult, studious and well spoken, and I quickly made progress as I reached out for privileges and responsibilities. I had no idea then that so many of those behaviors of people pleasing, finding worth in accomplishments and external accolades, perfectionism, and workaholism were due to growing up in alcoholic dysfunction. My Dad was an alcoholic who left us and the religion when I was little. (He has now been sober for more than 25 years and we have a great relationship.)
My parents divorced when I was 6. My Mom was a single parent until she married another alcoholic when I was 11. He was a belligerent domineering drunk. When I was a teenager and young adult, it was my religion that saved me from that. Being a “spiritual” person formed a core part of my identity. But by the time I came into AA, overloaded with commitments, no idea what self-care meant, in a broken marriage I felt I couldn’t leave, and in the early stages of serious alcoholism myself, I was completely disillusioned with my own religious belief system and my experiences within that religious community, especially when it came to dealing with my family and relationship problems.
When I started AA, I was neck-deep in comparative religion, Eastern and Western philosophy, and all kinds of academic pursuits related to theology, philosophy, psychology, and sociology – all the things I wasn’t allowed to explore growing up. I was in the process of deconstructing all of my former beliefs, trying to get behind and beyond the intense feelings of guilt and shame that I was experiencing as I found myself unable to believe, trying to detach from all the things I used to do as a believer and not realizing how much loss I was experiencing, and finally embracing the dissonance and the questioning and discarding certainty.
I became a heretic, an apostate, according to my former religion. I wore the label proudly, in the mood of Ambrose Bierce in The Devil’s Dictionary: “Apostate: a leech who, having penetrated the shell of a turtle only to find that the creature has long been dead, deems it expedient to form a new attachment to a fresh turtle.” I didn’t want a fresh turtle, I wanted to know what turtles were made of and whether there was anything real beyond more dead turtles. When I left my former religion, I never seriously considered joining some other religion, and I didn’t gravitate towards any “anti” group of former members of the one I had left. I also didn’t feel like a joiner with secular humanist groups or the more committed anti-religion atheists. I found AA plenty tolerant and open, though a few individuals could get a tad preachy for my liking. I mostly ignored them, recognizing in them much that seemed familiar from the thought world I had just left.
I brought a flippant, judgmental, but also intensely curious and serious energy into my AA recovery journey. I wasn’t even aware yet of the grief and loss I was about to go through leaving the worldview and community that I was raised in. The religious family trauma that happened then and continues to happen now is a mainstay of why I need recovery and the recovery community. It’s the ground I walk on, the air I breathe. So keeping AA open, welcoming, tolerant, and loving to all believers and unbelievers is important to me.
At the time I was coming into AA, words like “spiritual” were just… fraught. Loaded. There was a valence on them, a charge. Today they might be called “trigger” words. They were slippery. They meant too many different things. So, when I thought, and when I talked, I avoided them. I had heard a quote around that time by Wittgenstein: “The limits of my language mean the limits of my world.” I took that to mean that if I wanted to think beyond the boundaries of the little world I had been raised in, I needed to expand my language, and use different words than I was used to using to say what I meant. (I didn’t know that Wittgenstein might have meant that if you can’t say anything about something because it’s beyond language, then say nothing, because saying anything might just be nonsense.)
I needed to say what was worth saying in such a way that the completely uninitiated unbeliever and the devout believer would understand me. I didn’t realize then that I wasn’t actually doing that for other people, I was doing that for me. I needed to get to the heart of the matter with why AA worked for some people and not for others, because clearly (to me) that couldn’t be “God” in any conventional sense, unless I accepted that God was arbitrary and inconsistent and almost passive-aggressive and opaque. I didn’t accept that.
If there was some reality out there that some people referred to as “God” in the practice of the program of Alcoholics Anonymous, I wanted to be able to describe it and think about it in specific ways that didn’t need the extra ingredient “God”. I still had plenty of awe and wonder even so. It was at this time I discovered the book The Spirituality of Imperfection, by Ernest Kurtz and Katherine Ketcham, and that book made it possible for me to work the 12 Steps, including the ones with “God” in them, with a sponsor, and that changed my life.
When I listened to others, I did a lot of translating. That made me work harder to find meaning for myself, to pay attention to and honor the person’s experience as they shared, or to relate the deeper meaning or intent or principle that was being expressed to some other concept that made more sense for me. It became more and more clear to me that much of the religious language that people use is just shorthand for our shared, lived, human experience. It can be a way for people to express themselves in a way they think others will understand. I was healed from some of my loss and religious pain by getting other believers’ perspectives, because it showed me that many paths and many options were available, both within a given belief system, and outside of it.
I love the word spiritual, even though it’s a term I had to redefine for myself, and it’s a term that some of my friends in humanist circles dislike. Here’s what spiritual currently means to me as a mystical atheist, or whatever I am.
Connection with others based on honesty, openness, vulnerability, and mutual respect. To me, this is the heart of recovery. All the actions, all the friendships, all the community, everything works better when it’s coming from a place of openness and honesty. Getting real. Going deeper. This reminds me, constantly, that there’s something beyond me, whether that means beyond my ego and the stories I tell myself, somewhere deeper within my own consciousness and my own being; beyond my own individual understanding and resources and wisdom; or beyond my own denial, wishful thinking, or skewed picture of reality towards something more real, more whole, more accurate, more objective out there. That feeling of connectedness, and the results of actions that come from practicing it in my life, I will gladly call that spiritual.
Perennial cultural wisdom and the truth of experience. Recovery samples ‘the wisdom of the ages’ and sages right next to the wisdom of John, and Cathy, and Judy, and Dennis – or whoever happens to be there. The cultural wisdom of lived experience keeps recycling itself in settings where people famously use the word ‘God’ in one sentence and the word ‘fuck’ in the next. My experience in recovery constantly reinforces to me that this wisdom is not found exclusively in religious texts or movements, as I was taught growing up – but neither is it found exclusively outside of these sources, as I thought when I was leaving mine. Religion and religious beliefs work for some people. They just don’t work for me anymore, not in the same way. But hearing the truth of my life out of someone else’s mouth, that deep recognition and identification, and becoming aware of options and context and perspectives that I wasn’t able to get to all on my own – that I will gladly call spiritual, even if it’s purely psychological, purely social. Man is a social animal, and it turns out that wisdom can be found around other people, even a group of drunks.
Awareness of finiteness, limitation, temporality, and mortality. “Life on life’s terms” seems to me the best brief encapsulation of this. Hearing thousands of shares at hundreds of recovery meetings reminds me of the shared human condition. I am not helpless or hopeless, nor am I unique. I am like other people. And I am not in control of everything. Some people call this state of mind “humility” but that is also a loaded word for me. Sometimes this kind of awareness is a cause of childlike wonder and curiosity, openness, gentleness. Sometimes it’s terrifying, like when someone learns they have cancer. Sometimes it’s frustrating, annoying, disappointing. Sometimes it brings fear and anger and the desire to escape. But at the end of the day, this is what makes us human, this is what makes us more like each other than not, and this is the basis for compassion as well as an appreciation for beauty, for good, for joy, for serenity.
Human qualities of the heart, such as honesty, hope, courage, integrity, willingness, forgiveness, perseverance, and compassion. All of the best of human nature can be found in the human stories in the rooms, right alongside the worst. Our best and highest selves are always available, always something to reach for, to aspire to. To me they’re actually nearer the surface in a real place with real people having real struggles. As Leonard Cohen sang it, “There is a crack in everything, that’s how the light gets in.”
That’s mostly what I mean by spiritual experience or spiritual energy. I’ve also come to appreciate that all the “profane” ordinary things count too – nature, exercise, sports, nutrition, and so many other things that keep us relatively healthy and whole.
Once, after a particularly dark period in my life, in sobriety, I heard a voice say clearly and distinctly “you are stronger than you think.” I’m not one for hearing voices. It wasn’t God. It was my own inner resources, the ‘god within’, a part of my psyche. But it was still a spiritual experience. Recovery and everything that has come into my life since starting it have helped me become more and more aware of my own precious worth, and my own abilities and responsibilities. It’s up to me to apply what I’ve learned, ask for help, and do my best to create the life and world that I want to have for myself. It’s up to me. But I’m not alone. Recovery has helped me know that I can do it, that I am doing it. That’s a spiritual awakening, a coming into the fullness of life that I didn’t think was possible when I got here.
Thank god. Or as George Carlin used to say, “Thank Joe.”
Chad Minteer got sober in Twin Falls and Jerome, Idaho. He’s an aspiring writer and part-time blogger, when he’s not doing his day job managing mobile GIS software development for mosquito control field operations. He identifies as a member of Alcoholics Anonymous, but also is at home in Al-Anon, Adult Children of Alcoholics (ACA), and Codependents Anonymous (CODA).
Chad writes a recovery and travel blog at www.recoveringallofme.com, covering unpopular emotions like shame and anger, heterodox recovery, and any book, event, group, or program that supports free thought and emotional freedom connected with recovery. You can contact him through his website or at [email protected]. He’d be happy to consider covering your event or reviewing your book and writing about it or publishing your blog article on similar topics.
The featured image for today’s article is a photo taken by Robin J Ramage in Port Dover, Ontario.
As the coronavirus hit communities across the United States over the summer, four overnight camps in Maine successfully kept the virus at bay.
Of 1,022 people who attended the summer camps, which included campers and staff members, only three people tested positive for COVID-19, researchers report August 26 in the Morbidity and Mortality Weekly Report. That’s because the people who came to Maine from 41 U.S. states, Puerto Rico, Bermuda and five other countries diligently followed public health measures put in place to stop transmission, the team says.
The camps’ success, as well as others including child care programs in Rhode Island that limited coronavirus transmission, could point to a path forward for places like schools that are reopening with in-person classes in the face of the ongoing pandemic, though challenges remain.
At the camps, a combination of testing, social bubbles, social distancing, masks, quarantine and isolation prevented outbreaks.
Before arriving at camp, officials told all 642 children and 380 staff members to quarantine with their households for 10 to 14 days. Attendees were also tested for COVID-19 five to seven days prior to arrival — with the exception of 12 people who had already been previously diagnosed. Four people tested positive for the virus and isolated for 10 days at home before heading off to one of the camps, which were in session at different times from mid-June to mid-August. (Three of the four camps ran for less than 50 days and the other went on for 62 days.)
Once on site, the campers and staff participated in daily symptom checks and activities held largely outdoors. They also hung out in small “bubbles,” or cohorts, that ranged from five to 44 people in size and became like family during the weeks at camp, the researchers say. If people interacted with anyone outside their group, masks and social distancing were required.
“We wanted to give the kids the ability to have a family unit at camp that they didn’t need to be masked or social distanced from,” says Laura Blaisdell, a pediatrician at Maine Medical Center Research Institute in Scarborough who worked on the new report.
Attendees came to Maine via car, bus and plane, and could have been exposed to the virus after their initial test, so officials retested the 1,006 attendees who had never had COVID-19 four to nine days after their arrival.
In that round of testing, two staff members and one camper from three different camps tested positive but never developed symptoms. Their cohorts were quarantined for two weeks, but still “were able to have a camp experience … and continue to have fun and play together,” Blaisdell says. The three positive cases didn’t transmit the virus to anyone else before they were identified. They each remained isolated until they had two negative test results.
Off to camp
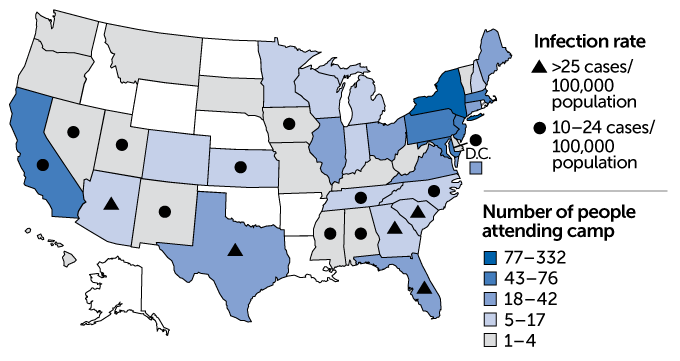
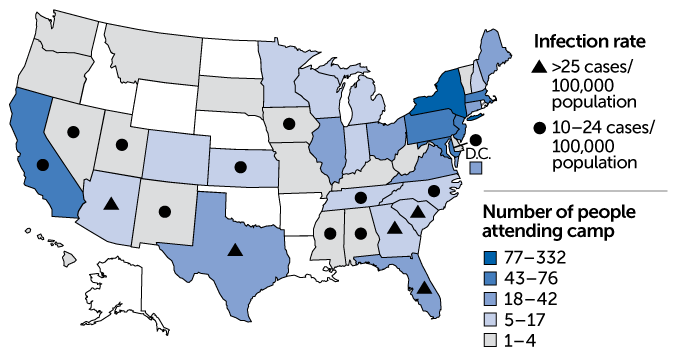
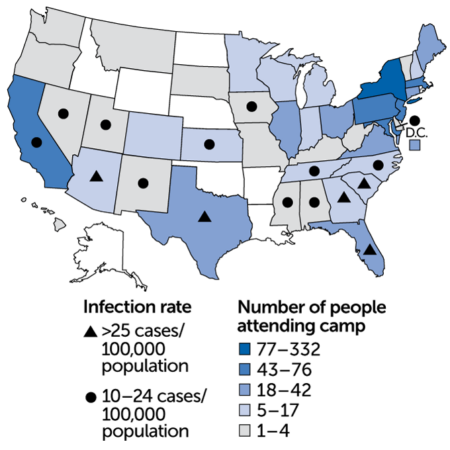
More than 1,000 people from 41 U.S. states, as well as Puerto Rico, Bermuda and several other countries, attended summer camps in Maine from mid-June to mid-August. The map shown here indicates which states campers and staff members came from. (No one attended from states colored white.) A fair number of people traveled from states like Texas and Florida that were hit hard over the summer (seven-day daily average rate of coronavirus infection as calculated on July 1, shown), but the camps’ public health measures prevented outbreaks. States with less than 10 cases per 100,000 population are not designated.
Camp population, by home state, and states’ COVID-19 infection rates
L.L. Blaisdell et al/MMWR 2020
L.L. Blaisdell et al/MMWR 2020
Some people traveled to Maine from areas where COVID-19 cases were surging over the summer, including Texas, Arizona and Florida. But rigorous testing quickly identified potential spreaders, and small cohorts allowed officials to quickly identify those most at risk of catching the virus.
In that way, “cohorting is an unsung hero of public health intervention,” Blaisdell says.
While interventions like cohorts, social distancing and wearing masks can help reduce coronavirus transmission on their own to some extent, each method has limitations. Combining such strategies into a layered approach where people follow multiple guidelines to curb the virus’ spread, like the Maine camps did, can further protect the members of a community.
“Every public health layer is like a layer of Swiss cheese with a hole in it,” Blaisdell says. It’s the stacking of “multiple layers of cheese on top of each other that close those holes and makes for a robust [infectious] disease plan.”
By contrast, a summer camp in Georgia faced an outbreak of the virus even after requiring attendees to provide proof of a negative test before arrival. But there, campers were not required to wear masks, weren’t tested after they arrived at camp and participated in both indoor and outdoor activities (SN: 7/31/20).
Still, the isolated nature of the summer camps in Maine likely made creating a relatively COVID-19–free bubble much easier than it might be at K–12 schools or universities around the country, where people come and go and may not live on site (SN: 8/4/20). There were some staff members at the four camps in Maine who went home every day, but those people were required to wear masks at all times and social distance from other attendees. It also likely helped that the amount of coronavirus circulating in Maine was quite low while the camps were running.
What’s more, the larger the school, the harder it will probably be to make sure that public health interventions are being adhered to. “If you follow the rules, then this can absolutely be successful,” says Brian Nichols, a virologist at Seton Hall University in South Orange, N.J. But, “when you scale it up and start looking at public schools and universities, you just have to plan on the fact that some people aren’t going to follow the rules.”
Nevertheless, the success in Maine hints that containing the virus is possible with a targeted, layered approach, Blaisdell says. “As schools and colleges begin to consider opening, they need to look at their community as a bubble,” she says. “We all need to be making contracts with each other about the behaviors that we’re going to do.”
August 20, 2020 – “The world we are proposing will significantly reduce the harm experienced by the most marginalized in our society and actually improve public and community health,” said Queen Adesuyi, a policy manager at DPA’s Office of National Affairs. “It will also reveal the truth—that the problem has never been drugs. After one of the largest political uprisings in history this year, maintaining the status quo is not as politically feasible as it might have been in the past.” Titled the Drug Policy Reform Act, the model bill’s many provisions including abolishing criminal penalties for drug possession, decarceration, expungement of drug criminal records, anti-discrimination measures, and reinvesting money into communities and drug-user health. It would give the power to categorize and regulate controlled substances, currently held by the Drug Enforcement Administration (DEA), to the National Institutes of Health (NIH) instead.
“Across the country and within the halls of Congress, it is becoming more and more common to hear elected officials speaking directly to the fact that drug use should not be treated as a criminal issue…
President Donald Trump accepted the Republican Party’s nomination for president in a 70-minute speech from the South Lawn of the White House on Thursday night.
Speaking to a friendly crowd that didn’t appear to be observing social distancing conventions, and with few participants wearing masks, he touched on a range of topics, including many related to the COVID pandemic and health care in general.
Throughout, the partisan crowd applauded and chanted “Four more years!” And, even as the nation’s COVID-19 death toll exceeded 180,000, Trump was upbeat. “In recent months, our nation and the entire planet has been struck by a new and powerful invisible enemy,” he said. “Like those brave Americans before us, we are meeting this challenge.”
At the end of the event, there were fireworks.
Our partners at PolitiFact did an in-depth fact check on Trump’s entire acceptance speech. Here are the highlights related to the administration’s COVID-19 response and other health policy issues:
“We developed, from scratch, the largest and most advanced testing system in the world.”
This is partially right, but it needs context.
It’s accurate that the U.S. developed its COVID-19 testing system from scratch, because the government didn’t accept the World Health Organization’s testing recipe. But whether the system is the “largest” or “most advanced” is subject to debate.
The U.S. has tested more individuals than any other country. But experts told us a more meaningful metric would be the percentage of positive tests out of all tests, indicating that not only sick people were getting tested. Another useful metric would be the percentage of the population that has been tested. The U.S. is one of the most populous countries but has tested a lower percentage of its population than other countries.
The U.S. was also slower than other countries in rolling out tests and amping up testing capacity. Even now, many states are experiencing delays in reporting test results to positive individuals.
As for “the most advanced,” Trump may be referring to new testing investments and systems, like Abbott’s recently announced $5, 15-minute rapid antigen test, which the company says will be about the size of a credit card, needs no instrumentation and comes with a phone app through which people can view their results. But Trump’s comment makes it sound as if these testing systems are already in place when they haven’t been distributed to the public.
“The United States has among the lowest [COVID-19] case fatality rates of any major country in the world. The European Union’s case fatality rate is nearly three times higher than ours.”
The case fatality rate measures the known number of cases against the known number of deaths. The European Union has a rate that’s about 2½ times greater than the United States.
But the source of that data, Oxford University’s Our World in Data project, reports that “during an outbreak of a pandemic, the case fatality rate is a poor measure of the mortality risk of the disease.”
A better way to measure the threat of the virus, experts say, is to look at the number of deaths per 100,000 residents. Viewed that way, the U.S. has the 10th-highest death rate in the world.
“We will produce a vaccine before the end of the year, or maybe even sooner.”
It’s far from guaranteed that a coronavirus vaccine will be ready before the end of the year.
While researchers are making rapid strides, it’s not yet known precisely when the vaccine will be available to the public, which is what’s most important. Six vaccines are in the third phase of testing, which involves thousands of patients. Like earlier phases, this one looks at the safety of a vaccine but also examines its effectiveness and collects more data on side effects. Results of the third phase will be submitted to the Food and Drug Administration for approval.
The government website Operation Warp Speed seems less optimistic than Trump, announcing it “aims to deliver 300 million doses of a safe, effective vaccine for COVID-19 by January 2021.”
And federal health officials and other experts have generally predicted a vaccine will be available in early 2021. Federal committees are working on recommendations for vaccine distribution, including which groups should get it first. “From everything we’ve seen now — in the animal data, as well as the human data — we feel cautiously optimistic that we will have a vaccine by the end of this year and as we go into 2021,” said Dr. Anthony Fauci, the nation’s top infectious diseases expert. “I don’t think it’s dreaming.”
“Last month, I took on Big Pharma. You think that is easy? I signed orders that would massively lower the cost of your prescription drugs.”
Quite misleading. Trump signed four executive orders on July 24 aimed at lowering prescription drug prices. But those orders haven’t taken effect yet — the text of one hasn’t even been made publicly available — and experts told us that, if implemented, the measures would be unlikely to result in significant drug price reductions for the majority of Americans.
“We will always and very strongly protect patients with preexisting conditions, and that is a pledge from the entire Republican Party.”
Trump’s pledge is undermined by his efforts to overturn the Affordable Care Act, the only law that guarantees people with preexisting conditions both receive health coverage and do not have to pay more for it than others do. In 2017, Trump supported congressional efforts to repeal the ACA. The Trump administration is now backing GOP-led efforts to overturn the ACA through a court case. And Trump has also expanded short-term health plans that don’t have to comply with the ACA.
“Joe Biden recently raised his hand on the debate stage and promised he was going to give it away, your health care dollars to illegal immigrants, which is going to bring a massive number of immigrants into our country.”
This is misleading. During a June 2019 Democratic primary debate, candidates were asked: “Raise your hand if your government plan would provide coverage for undocumented immigrants.” All candidates on stage, including Biden, raised their hands. They were not asked if that coverage would be free or subsidized.
Biden supports extending health care access to all immigrants, regardless of immigration status. A task force recommended that he allow immigrants who are in the country illegally to buy health insurance, without federal subsidies.
“Joe Biden claims he has empathy for the vulnerable, yet the party he leads supports the extreme late-term abortion of defenseless babies right up to the moment of birth.”
This mischaracterizes the Democratic Party’s stance on abortion and Biden’s position.
Biden has said he would codify the Supreme Court’s ruling in Roe v. Wade and related precedents. This would generally limit abortions to the first 20 to 24 weeks of gestation. States are allowed under court rulings to ban abortion after the point at which a fetus can sustain life, usually considered to be between 24 and 28 weeks from the mother’s last menstrual period — and 43 states do. But the rulings require states to make exceptions “to preserve the life or health of the mother.” Late-term abortions are very rare, about 1%.
The Democratic Party platform holds that “every woman should have access to quality reproductive health care services, including safe and legal abortion — regardless of where she lives, how much money she makes, or how she is insured.” It does not address late-term abortion.
PolitiFact’s Daniel Funke, Jon Greenberg, Louis Jacobson, Noah Y. Kim, Bill McCarthy, Samantha Putterman, Amy Sherman, Miriam Valverde and KHN reporter Victoria Knight contributed to this report.
Feelings of panic when a person is away from their smartphone could be connected to general feelings of inadequacy and inferiority, a new study of young people in Portugal suggests.
A researcher slips stickers under some colored cups on a lazy Susan, then gives the tray a whirl. When the spinning stops, a preschooler must find the hidden stickers. Most children remember where the stickers are, but a few have to check every single cup.
The game tests working memory, which is among the set of mental skills known as executive function that can be impaired in children who faced trauma early in life.
Adversity wreaks havoc, and from there, “you have a system that responds differently,” says Megan Gunnar, a developmental psychobiologist at the University of Minnesota in Minneapolis who has spent two decades studying the impact of early-life adversity in adopted children. The focus of this work is extreme adversity, such as being orphaned, rather than everyday challenges, which might teach beneficial resilience.
A childhood characterized by hardship, negligence or abuse can also alter the neuroendocrine system that regulates how the body responds to stress. Problems in the stress response can set kids on a path toward behavior struggles along with increased risk for depression, diabetes and a host of other health problems.
But recent studies offer hints that such a difficult future may not be inevitable. As Gunnar and others have shown, impaired stress responses can return to normal during puberty, raising the possibility that imbalances created by early trauma can be erased. The research is prompting a new view of puberty as an opportunity — a chance for people who had a shaky start to reset their physiological responses to stress.
A sense of safety
When the brain perceives a threat — even a temporary one such as a stressful exam or a high-stakes competition — levels of the hormone adrenaline shoot up, setting off the “fight-or-flight” reaction. Breathing and heart rate soar. Palms get sweaty. Sight and other senses sharpen. Before long, the brain sends chemical messengers to stimulate adrenal glands near the kidneys to release cortisol.
A spin-the-pots task, with colored cups and hidden stickers, tests working memory, which can be impaired in children who experience early hardship.N.H. Brito et al/Frontiers in Psychology 2014
Cortisol sends sugars into the blood for quick energy. The hormone also slows digestion, immune responses, growth and other processes considered nonessential in a fight-or-flight situation.
When the threat passes, the fight-or-flight response ends, at least in a person whose stress response is working as it should. Adrenaline and cortisol levels fall, heart rate slows and other systems resume business as usual.
When Gunnar started her doctoral work in the 1970s, researchers had already mapped out the key actors in the stress response. The neuro-endocrine signals involved form the HPA axis, short for hypothalamic-pituitary-adrenal. When rodents and monkeys face early-life adversity, the HPA axis gets thrown off-kilter. As methods became available for measuring cortisol from samples of saliva — rather than having to collect blood or urine — Gunnar set out to study how the HPA axis influences the brain and behavior in humans.
From experiments with newborn babies in the mid-1980s, Gunnar showed that having a secure parent relationship is important for a healthy neuroendocrine system and helps babies deal with stressful situations, such as getting immunizations. “You can go to the doctor as a baby and get a big shot in one leg and the other leg, and you’re crying your head off … but [the HPA axis] doesn’t kick off,” Gunnar says. However, shots or no shots, if babies get separated from their parents for even a few minutes, “their HPA axis shoots up like a rocket.”
Gunnar wondered what happens if that sense of safety is disrupted longer-term. She tried studying maltreated and impoverished children, but separating the effects of early hardship from later difficulties is not easy. “The way you start out in life tends to continue,” Gunnar says. A report published last November by the U.S. Centers for Disease Control and Prevention points to the long-term consequences: Compared with their peers, adults who experienced childhood trauma are more likely to smoke, drink heavily, have dropped out of high school and develop heart disease and a host of other chronic conditions.
A trip in the mid-1990s set Gunnar on a new path to answer that tricky research question. She ventured with a research team to an orphanage in eastern Romania, where young children were raised in overcrowded, inhumane conditions. “You walk into these wards, and all of a sudden you’re mobbed by kids saying ‘Mama, mama, mama’ … reaching their arms up to get held,” says Gunnar, who had two school-age sons at the time. “It was awful. I just wanted to bring them all home.”
What she did bring back to Minnesota, along with that searing memory, was a set of small vials, each containing a saliva sample from a 2- or 3-year-old orphan. To her surprise, the children’s cortisol levels — the end product of the neuroendocrine cascade — were lower than the average toddler’s. That finding offered a window into the effects of long-term parental deprivation on stress responses.
Adoptee struggles
To single out the effects of early hardship, Gunnar needed children who had started life in deprivation but then moved into healthy, supportive environments after infancy. Such children would be the ideal human analog for all of the animal studies on early adversity, she thought. It dawned on her that this group exists: adopted orphans.
Gunnar shared her idea with members of the adoption unit at the Minnesota Department of Human Services. With the department’s support and funding, she surveyed Minnesota parents who had adopted children internationally in the 1990s, and invited families to join a university registry and participate in research.
Many parents in the study had noticed early on that their adopted children had behavioral problems. And when the youngsters came to the university lab for problem-solving and sorting tests, including the lazy Susan task and the famous marshmallow test of delayed gratification (SN: 8/4/18, p. 14), the children struggled with attention and self-regulation.
Like the Romanian orphans, these kids had lower cortisol levels than nonadopted children who had no behavioral problems. In the face of sustained hardship, which has the potential to encourage dangerously high levels of cortisol, a weak stress response — that is, producing less cortisol — could be “nature’s way of preserving the brain and body,” Gunnar speculates.
Teen-time shift
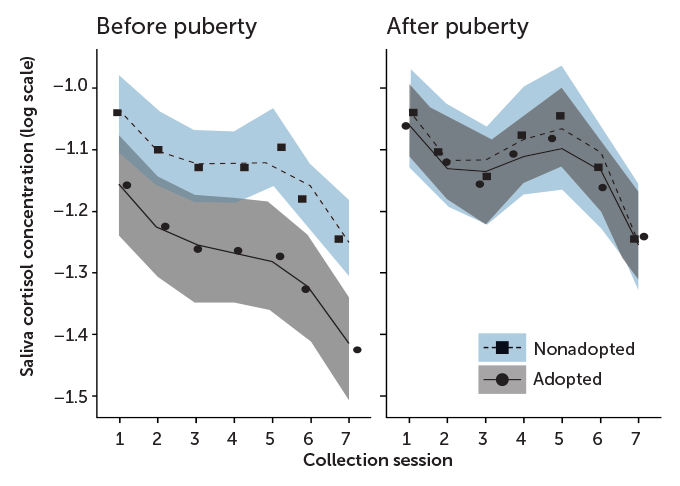
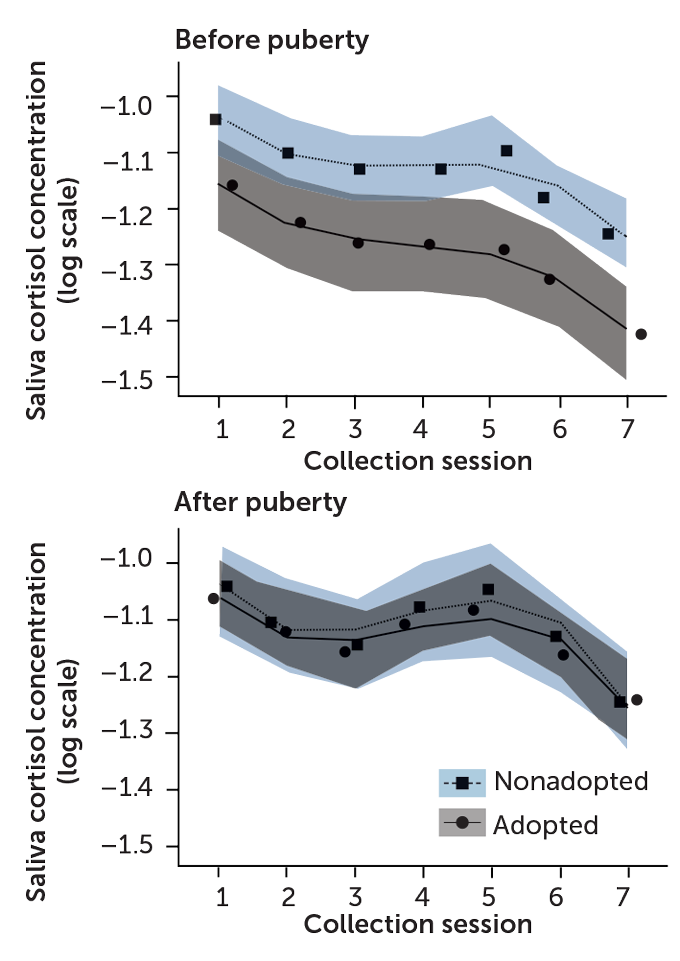
Before puberty, adopted children, who grew up with early-life trauma (gray curve), had blunted stress responses relative to kids living with biological parents (blue curve). By the time puberty ended, the adopted children showed normal cortisol patterns before, during and after a stressful task. Saliva was collected 20 minutes and 5 minutes before the task, then 5, 20, 40, 60 and 80 minutes after the task. The researchers converted the data to a logarithmic scale, which shows negative numbers. The actual cortisol levels are between 0 and 1 micrograms per deciliter.
Cortisol stress response in adopted and nonadopted children
T. Tibbitts
T. Tibbitts
Source: C.E. DePasquale, B. Donzella and M.R. Gunnar/J. Child Psychol. Psychiatry 2019
Studying the adoptees over time, she found that preschoolers with low cortisol often entered kindergarten with attention problems. A blunted stress response persisted into middle childhood, even after an average of seven to eight years in a household with healthy caregiving.
That was disheartening, says Russell Romeo, a psychobiologist at Barnard College in New York City. “We’d always thought that maybe if these individuals get out of the adverse situations, they could start recalibrating their stress reactivity.”
But research Romeo had done in the mid-2000s gave Gunnar reason to think she just needed to look further down the road of the children’s lives.
High time for change
Romeo was studying rats to see if stress affects adolescent and adult brains differently. In one set of experiments, he subjected adult rats and prepubescent rats to acute stress — 30 minutes trapped inside a wire mesh container — and recorded their levels of corticosterone (the rat version of cortisol) before, during and after the confinement. Both groups produced similar hormone spikes when stressed, but in the juvenile rats, levels took much longer to return to normal.
When Romeo observed how the animals reacted to extended periods of stress — 30 minutes of restraint each day for seven days — the pattern was different. After the animals were released from the restraints, stress hormones surged higher in young rats than in adults. But the rats that were near puberty returned to baseline more quickly than the older animals. Taken together, Romeo’s studies suggested that neuroendocrine stress responses get shaped during puberty to emerge differently in adulthood.
In earlier work, researchers at McGill University in Montreal showed that moving adolescent rats into “enriched” environments — larger cages with more toys and cagemates — could reset stress responses that had been thrown out of whack by early-life trauma.
These findings heartened Gunnar. “Maybe I should be looking at puberty,” she thought. It could be a time to recalibrate.
Closer to normal
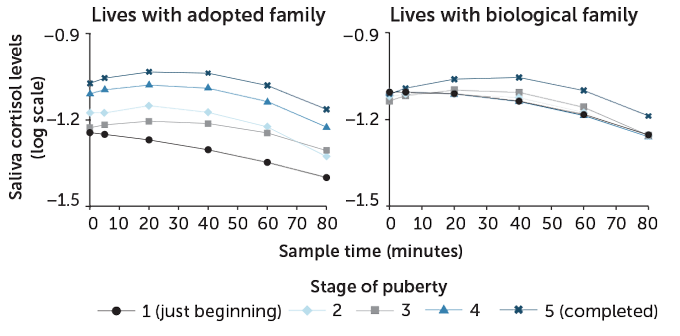
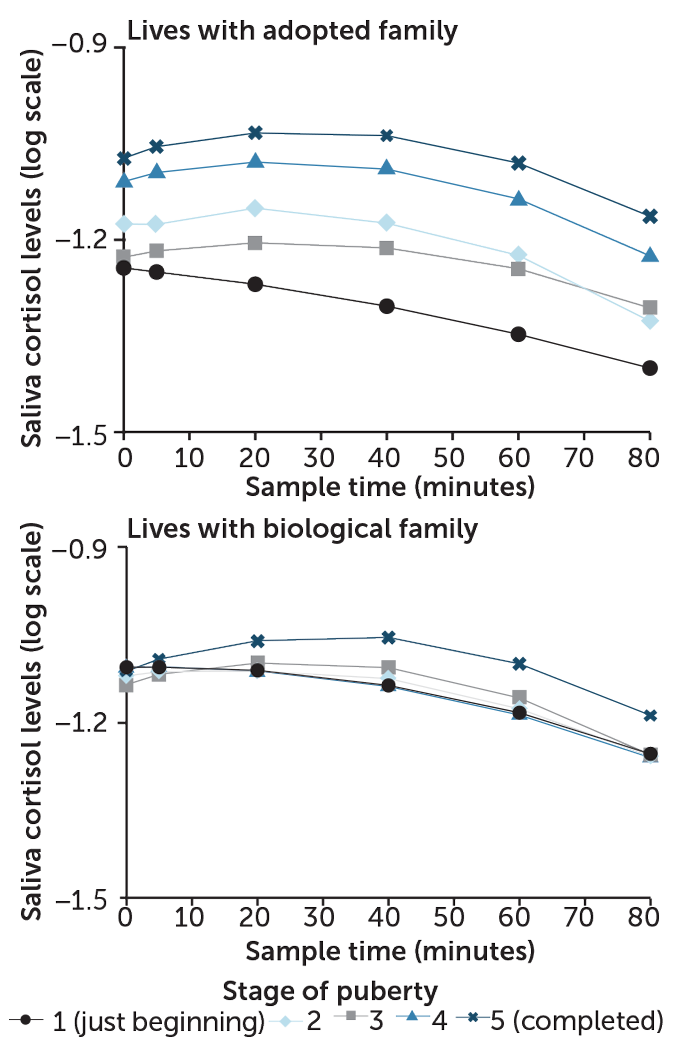
During a stressful activity (giving a speech, for example), saliva cortisol levels rose temporarily and returned to normal in those children who lived with their biological parents. Children who were adopted after starting life in an orphanage (an early-life trauma), had blunted cortisol responses during stages 1 to 2 of puberty. But at the tail end of puberty, stages 4 and 5, adopted children’s stress responses normalized.
Stages of puberty and cortisol stress reaction
T. Tibbitts
T. Tibbitts
Source: M.R. Gunnar et al/PNAS 2019
So her team invited 280 7- to 14-year-olds — 122 children adopted from institutions and 158 from socioeconomically comparable biological families — into the lab to complete two stressful tasks. One involved challenging mental math. For the second task, each child prepared a five-minute speech introducing themselves to a new class of students. The children were told that their speech, given in front of a video camera and a mirror, would be rated by judges. Some kids spoke with confidence, while others looked nervous. “We did have one who burst into tears,” Gunnar says. But “we don’t torture them. If we think they’re too nervous, we help them quit.”
Before and after the speech and math tasks, researchers collected saliva samples from each child to measure cortisol levels. Participants’ pubertal status was assessed on a 1-to-5 scale: Stage 1 meant no noticeable body changes and stage 5 meant sexual maturation was complete.
Among kids in early puberty (stages 1–2), adopted kids had blunted cortisol levels before and after the tasks compared with children who lived with their biological parents. This result confirmed Gunnar’s previous research on preschool-aged international adoptees. In the late puberty group (stages 4–5), cortisol patterns looked similar for adopted and nonadopted kids.
To confirm HPA recalibration had occurred within the same child, rather than just comparing across age groups, Gunnar and colleagues brought participants in for the same tests one and two years later, for a total of three annual sessions.
The results, reported in the Nov. 26 Proceedings of the National Academy of Sciences, show the body can recalibrate its response to stressors during puberty. In other words, something happens in puberty — but not earlier in childhood — that allows the brain to shift back to normal stress responses that had been skewed by early trauma.
Matthew Duggan, a therapist in Long Beach, Calif., who specializes in childhood and adolescence, is encouraged by the findings and thinks they could apply to a wide range of children who have trouble managing their emotions and connecting with others because caretakers abused or ignored them early in life. There may be “a window … where things might be able to change,” Duggan says. “And we have some data here to suggest that at a biological level, that is a possibility. For me, that’s really hopeful to see.”
Duggan says Gunnar’s study would have been even more useful if it had assessed participants’ behavior change — for example, by interviewing parents, teachers or the adolescents themselves.
How might puberty combine with better caregiving and support to reshape neuroendocrine stress responses? Romeo speculates that it stems from the fact that the hypothalamus and other brain areas, such as the prefrontal cortex, that control our reactions to stress are among the regions that rewire and strengthen connections during adolescence.
Whether those changes in the stress response will ultimately harm or help a young person is hard to predict, Gunnar says. Mental health and resilience emerge from an ever-changing combination of genes and life experiences — some of which set the body awry early on. But adolescence could potentially erase some of the damage, her research shows. Gunnar and others hope to reveal more of the underlying biology behind the reboot.
Is there a sweet spot for early adversity?
Hardships early in life can mean a difficult road ahead. But some small amount of stress may help kids build mental toughness to handle the stresses of everyday life, such as big exams or performances (SN: 6/8/19, p. 12).
“We learn to handle stress by handling stress,” says Megan Gunnar, a developmental psychobiologist at the University of Minnesota in Minneapolis.
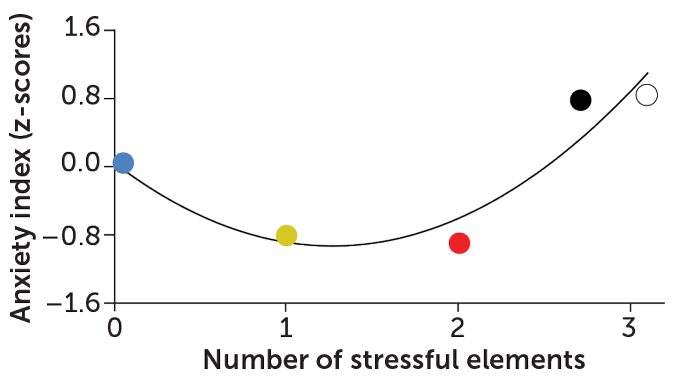
Early-life stress affects later resilience
T. Tibbitts
Groups of lab monkeys exposed to mild or moderate stress (yellow and red dots) showed lower anxiety later than animals exposed to no stress (blue) or heavy stress (black and white).
Source: K.J. Parker et al/Scientific Reports 2019
If a stressful experience shows “the world is tough but we can deal with it, perhaps with the help of family and friends,” she says, “we are tougher the next time.” On the other hand, feeling crushed by an intense stressor, such as abuse or a parent’s death, can impart a sense of helplessness that leaves young people “fearful of it happening again,” Gunnar says.
In a 2010 study, researchers surveyed 2,398 U.S. adults to understand how pain and stress affect resilience. Participants answered questions about their mental health and overall well-being, and indicated whether they had experienced cumulative lifetime adversities, including a serious illness or divorce in the family. The upshot: People who faced some adversity reported less distress and more life satisfaction compared with those who either experienced heavy adversity or sailed through childhood with ease.
Experiments in monkeys suggest that this is more than a correlation. A team led by David Lyons, a behavioral neuroscientist at Stanford University, reported causal evidence last November in Scientific Reports. Since it can be unethical to randomly assign humans to stressful conditions, the team tested the effects of varying “doses” of stress in squirrel monkeys that had not yet reached puberty.
The monkeys in the control group enjoyed a typical lab life — housed in a cage with mom and siblings, plus plenty of water, food and toys. A second group faced a mild stressor — one hour of separation from siblings once daily for 10 days. The stress dose went up a notch for the third group, which had daily separation from siblings and no access to mom during that hour. Two additional groups experienced daily separation from mother and siblings, plus an injection as an additional stressor.
Ten weeks later, each monkey was moved with its mother to an unfamiliar cage. The researchers assessed the monkeys’ willingness to let go of mom and explore the new digs. The team also analyzed blood levels of the stress hormone cortisol before and after the time spent in the new cage. On the whole, monkeys in the groups that faced one or two stressors clung less to their mothers and more readily explored their new surroundings — showing less anxiety — than both the no-stress and the two high-stress groups.
Cortisol patterns also reflected this trend: Cortisol levels were closer to normal in monkeys exposed to mild or moderate stress than in monkeys from the other groups.
Growing up healthy means “learning how to deal with mild challenge and change,” Lyons says.






 I grew up as a Jehovah’s Witness and stayed until I was almost 30, about the time I started on my recovery path. I was a good little boy and young adult, studious and well spoken, and I quickly made progress as I reached out for privileges and responsibilities. I had no idea then that so many of those behaviors of people pleasing, finding worth in accomplishments and external accolades, perfectionism, and workaholism were due to growing up in alcoholic dysfunction. My Dad was an alcoholic who left us and the religion when I was little. (He has now been sober for more than 25 years and we have a great relationship.)
I grew up as a Jehovah’s Witness and stayed until I was almost 30, about the time I started on my recovery path. I was a good little boy and young adult, studious and well spoken, and I quickly made progress as I reached out for privileges and responsibilities. I had no idea then that so many of those behaviors of people pleasing, finding worth in accomplishments and external accolades, perfectionism, and workaholism were due to growing up in alcoholic dysfunction. My Dad was an alcoholic who left us and the religion when I was little. (He has now been sober for more than 25 years and we have a great relationship.) Chad Minteer got sober in Twin Falls and Jerome, Idaho. He’s an aspiring writer and part-time blogger, when he’s not doing his day job managing mobile GIS software development for mosquito control field operations. He identifies as a member of Alcoholics Anonymous, but also is at home in Al-Anon, Adult Children of Alcoholics (ACA), and Codependents Anonymous (CODA).
Chad Minteer got sober in Twin Falls and Jerome, Idaho. He’s an aspiring writer and part-time blogger, when he’s not doing his day job managing mobile GIS software development for mosquito control field operations. He identifies as a member of Alcoholics Anonymous, but also is at home in Al-Anon, Adult Children of Alcoholics (ACA), and Codependents Anonymous (CODA).