El presidente Donald Trump, que parece decidido a anunciar una vacuna para COVID-19 antes del día de las elecciones, podría autorizarla legalmente a pesar de las objeciones de expertos, funcionarios de la Administración de Alimentos y Medicamentos (FDA) e incluso los fabricantes, que se han comprometido a no lanzar nada a menos que haya demostrado ser seguro y eficaz.
En podcasts, foros públicos, redes sociales y revistas médicas, un número creciente de líderes de salud dicen que temen que Trump, quien ha señalado repetidamente su deseo de que la vacuna se apruebe rápido, tomará el asunto en sus manos, pasando por alto el proceso habitual.
Esto reflejaría otro intento por inyectar política en decisiones sensibles de salud pública. Trump ha contradicho repetidamente el consejo de científicos de alto nivel sobre COVID-19 y ha avalado tratamientos controversiales para tratar la enfermedad.
Las preocupaciones se intensificaron durante este fin de semana, después que Alex Azar, secretario de Salud y Servicios Humanos (HHS), afirmara la autoridad de su agencia sobre la FDA para establecer normas.
La FDA suele aprobar las vacunas. Pero Azar, que informa directamente a Trump, puede emitir una autorización de uso de emergencia, incluso antes que se haya demostrado que la vacuna es segura y eficaz en ensayos clínicos en etapa avanzada.
“Sí, este escenario es ciertamente posible legal y políticamente”, afirmó el doctor Jerry Avorn, profesor de medicina en la Escuela de Medicina de Harvard, quien describió este escenario en el New England Journal of Medicine. Dijo que “parece más aterrador y posible cada día”.
Expertos en vacunas y funcionarios de salud pública están particularmente molestos por la posibilidad porque podría arruinar la frágil confianza del público en una vacuna para COVID-19. Podría poner a las autoridades científicas en la posición de instar a las personas a no vacunarse después de años de intentar persuadir a los padres indecisos para que ignoraran temores infundados.
Los médicos podrían negarse a administrar una vacuna aprobada con datos inadecuados, dijo el doctor Preeti Malani, director de salud y profesor de medicina en la Universidad de Michigan en Ann Arbor, en un seminario virtual. “Podrías tener una vacuna segura y eficaz que nadie quiera usar”.
Judd Deere, vocero de la Casa Blanca, desestimó las preocupaciones de los científicos y dijo que a Trump solo le importaba la seguridad y la salud del público.
Por lo general, la FDA aprueba las vacunas solo después que las empresas presentan años de datos que demuestran que una vacuna es segura y eficaz. Pero una ley de 2004 permite a la FDA emitir una autorización de uso de emergencia con mucha menos evidencia, siempre que la vacuna “pueda ser efectiva” y sus “beneficios conocidos y potenciales” superen sus “riesgos conocidos y potenciales”.
Muchos científicos dudan que una vacuna pueda cumplir con esos criterios antes de las elecciones. Pero los términos pueden ser lo suficientemente vagos desde el punto de vista legal como para permitir que la administración tome tales medidas.
Moncef Slaoui, asesor científico jefe de Operation Warp Speed, el programa gubernamental que apunta a desarrollar más rápidamente las vacunas para COVID-19, dijo que es “extremadamente improbable” que los resultados del ensayo de una vacuna estén listos antes de finales de octubre.
Sin embargo, Trump ha insistido repetidamente en que a partir del próximo mes se distribuirá una vacuna para combatir la pandemia que ya se ha cobrado cerca de 200,000 vidas en el país. Reiteró esa afirmación el sábado 19 de septiembre en un mitín de campaña en Fayetteville, Carolina del Norte.
La vacuna estará lista “en cuestión de semanas”, dijo. “Pondremos fin a la pandemia de China”.
Aunque compañías farmacéuticas han lanzado tres ensayos clínicos en los Estados Unidos, nadie puede decir con certeza cuándo tendrán suficientes datos para determinar si las vacunas son seguras y efectivas.
Los funcionarios de Moderna, cuya vacuna se está probando en 30,000 voluntarios, han dicho que sus estudios podrían producir resultados para fin de año, aunque el análisis final podría realizarse la próxima primavera.
Los ejecutivos de Pfizer, que han ampliado su ensayo clínico a 44,000 participantes, aseguran que sabrán si su vacuna funciona a finales de octubre.
El ensayo de la vacuna de AstraZeneca en los Estados Unidos, que estaba programado para inscribir a 30,000 voluntarios, está entre paréntesis por una posible enfermedad relacionada con la vacuna.
Los científicos han advertido por meses que la administración Trump podría intentar ganar las elecciones con una “sorpresa de octubre”, autorizando una vacuna que no haya sido completamente probada.
En un artículo de opinión publicado en The Wall Street Journal, los ex comisionados conservadores de la FDA, Scott Gottlieb y Mark McClellan, argumentaron que la intrusión presidencial era poco probable porque el “proceso completo y transparente de la FDA no se presta a la intromisión. Cualquier desviación se haría evidente muy rápido”.
Pero la administración ha demostrado su voluntad de doblegar a la agencia a su voluntad. La FDA ha sido criticada por emitir autorizaciones de emergencia para dos tratamientos de COVID-19 que fueron impulsados por el presidente, pero que carecían de evidencia sólida que los respaldara: la hidroxicloroquina y el plasma convaleciente.
Azar ha dejado de lado a la FDA de otras maneras, como impidiendo que la agencia regule las pruebas desarrolladas en laboratorio, incluidas las del nuevo coronavirus.
Aunque el comisionado de la FDA, Stephen Hahn, le dijo al Financial Times que estaría dispuesto a aprobar el uso de emergencia de una vacuna antes de que concluyeran los estudios a gran escala, los funcionarios de la agencia también se han comprometido a garantizar la seguridad de cualquier vacuna para COVID-19.
El doctor Peter Marks, alto funcionario de la FDA que supervisa las aprobaciones de vacunas, ha dicho que renunciará si su agencia aprueba una vacuna para COVID-19 que no esté bien probada.
“Creo que habría una protesta insuperable de la comunidad de salud pública, que es mi peor pesadilla, mi peor pesadilla, porque confundiremos al público”, dijo el doctor Michael Osterholm, director del Centro de Investigación de Enfermedades Infecciosas y Políticas en la Universidad de Minnesota, en su podcast semanal.
Aún así, “incluso si una empresa no quisiera que se hiciera, incluso si la FDA no quisiera que se hiciera, él podría hacerlo”, dijo Osterholm, en su podcast. “Espero que nunca veamos que eso suceda, pero tenemos que considerar que es una posibilidad”.
En el editorial del New England Journal, Avorn y el coautor, el doctor Aaron Kesselheim, se preguntaron si Trump podría invocar la Ley de Producción de Defensa de 1950 para obligar a las farmacéuticas reacias a fabricar sus vacunas.
Pero Trump tendría que demandar a una empresa para hacer cumplir esta ley, y la empresa tendría un caso sólido para negarse, dijo Lawrence Gostin, director del Instituto O’Neill para la Ley de Salud Nacional y Global de Georgetown.
Además, señaló que Trump no podría invocar la ley a menos que una vacuna estuviera “científicamente justificada y aprobada por la FDA”.
Thank the Lord (in a manner of speaking) for the wonderful liberals among the God-believers in Alcoholics Anonymous as I encountered them years ago. These delightful creatures were more interested in seeing me get sober than in coaxing me into a new relationship with the Almighty. Alcoholics Anonymous provides the narrowest of gates for some of us. I remain genuinely grateful for the broad-minded folks who helped me to slither through.
The members of AA are a diverse group, of course. There were then and are now, many of a different ilk. The “Get God or die” proclaimers are alive and well and in most instances, they loudly vocalize their pronouncements of what PRECISELY needs to be done to get sober. As they see it, that involves suiting up for the “God could and would if he were sought” team.
The inimitable Joe C. of Toronto and I have more than once discussed AA’s decreasing inclusiveness over the past few decades. That unfortunate development has been closely tied to a resurgence of interest in our society’s now eighty-one year old text, and the spread of “Thumperism.”
Ten years ago, the late conference speaker Sandy Beach, anonymously penned a screed against atheists and agnostics in AA. In his “WHITE PAPER ON THE MATTER OF AA ATHEIST/AGNOSTIC GROUPS AND RELATED CONCERNS,” Mr B. let it be known that heathens could quietly take up membership in AA, but they needed to shut the Hell up about their non-conforming beliefs. That rambling discourse brought to mind the odd position taken up by the U.S. military regarding members of the LGBTQ community. “Please afford us the opportunity for plausible deniability. We’d like to go on pretending that you’re not even here.”
In “The ‘Don’t Tell’ Policy in AA” one of the finest essays ever to appear on this website, Roger C. looks at the similarity to AA in the U.S. military’s “Speak No Evil” stance.
Freethinkers in AA have been anything but silent in the twenty-first century. They are writing books, starting groups, and speaking out. The growth of the secular demographic in recent years has been remarkable. Closet atheists and agnostics have exited their armoires and are breathing the fresh air of free expression. Most recently, Zoom has brought the idea of non-religious AA to folks who otherwise could not have imagined such things.
Sorry, Sandy.
Of course, the fundies have been inspired to push back — hence the polarization.
But let’s return to the liberals. Those generous folks offered me a navigable path to sobriety. Forgive the cliches, but I was invited to replace the rejected God of my understanding with various G-O-D’s that included “Good Orderly Direction,” and “Group of Drunks.” Uncapitalized “higher powers” were offered for my consideration. The closest of my new friends made little effort to convert me.
Regarding my uncontrollable drinking, I was open to accepting the help of those who had overcome problems with alcohol that were similar to my own. I came to see a benefit in confession, restitution, helping others, and blending myself into the AA community. Earlier, I had come to a full acceptance that there is no path to moderate drinking for people like me and that quitting drinking on one’s own is a very tall order. The substitutions for God had not been presented to me as temporary measures, but many of my new friends were surprised that years of AA sobriety resulted in no alteration of my “Big Picture” worldview.
The Bigga Booka
The literature presents a different picture.
For the sake of brevity, I will bypass the 12 + 12 with its “Seven Deadly Sins” etc., to focus exclusively on the Bigga Booka, as my North Bay friend Lena likes to call the divinely-inspired source of all wisdom. The root of the popular “higher power” term is found in AA’s second step: “Came to believe that a Power greater than ourselves could restore us to sanity.” The liberals had told me that there were a lot of powers greater than me including alcohol. Employers, police, judges and wives were also mentioned.
It did not escape my notice that none of those “powers” come with capital “P’s.” Did any of these come with power sufficient to restore human beings to sanity? As it turns out, the somewhat liberal-sounding “Power greater” has a very brief shelf life. This temporary power is a mere place-holder – a set of training wheels shortly to be discarded. Those paying close attention were warned of this early in the book: “It was only a matter of being willing to believe in a Power (capital “P”) greater than myself. Nothing more was required of me to make my beginning. I saw that growth could start from that point.” (BB, p. 12, Bill’s Story)
On page 46, the pretense that “Power greater” and “God” are something different is dropped: “… it was impossible for any of us to fully define or comprehend that Power which is God.”
Presto Change-o
Magicians have some very cool names for their trickery – “prestidigitation,” “misdirection,” “legerdemain,” “hocus pocus,” “sleight of hand.” A distraction is created to disguise what’s really going on. While the left hand is doing something dramatic and eye-catching, the right hand engages in something sneaky. “Power greater” and “own conception of God” are left hand activities. The right hand is the Hand of God. It was there all along. In the literature, these issues are quite transparent. The “non-God” God option is a temporary measure – a single step onto Jacob’s ladder.
The agnostic, or atheist (God forbid), is expected to come around “sometimes quickly, sometimes slowly.” Look at “Our Southern Friend” Fitz, New York Number 3. The minister’s son had abandoned the religion of his childhood after finding it incompatible with his taste for hedonistic “sinning.” A mere half-hour after being visited by Bill and Hank, Fitz finds himself on his knees crying and praying, his “militant” atheism seemingly poofed away by the Grace of God.
(I am contemplating a lawsuit against the English department of the University of Toronto as I appear to have developed a very poor understanding of words like “militant.”)
Some of AA’s self-declared “militant atheists” were angry at God. Others such as Fitz were fearful of the divine wrath destined to come as retribution for his “sins of the flesh.” It was wishful thinking that perhaps the punishing God of his Christian upbringing was mythological. The mislabelers have contributed to the poor understanding of the “real” atheist and the educated agnostic in Alcoholics Anonymous circles.
The personal story of Bill’s book-producing business partner, Hank P., was called “The Unbeliever.” He too found himself bawling and praying to what he called a “Universal Power.” Although God was likely pleased by the capital letters, He may have found the mislabeling offensive, as He reversed Hank’s awakening and returned him to drinking less than five months after the Bigga Booka came to print.
Alcoholics Anonymous employs the magician’s chicanery although a word search of the sacred text reveals no “abracadabra’s.” They are implicit, I suppose.
My new AA friends had performed all manner of liberal-sounding misdirection. Most were sincere in their inclusiveness as they sought to change my drinking moreso than my philosophy. Their liberal talk is not backed up by the literature. The book is far more supportive of the fundamentalist’s position. “Get God or die.” “no human power,” etc.
The magician’s left hand holds up the “own conception” idea for the briefest time before we are presented with AA’s conception — the “real” view of what God is. He is omnipotent, benevolent, an Employer, a Father, a Director, a Manager, and a Him. We are suddenly smothered by an avalanche of “He’s” and “Him’s.” The female fundamentalist is forced to bite her lip and say, “It’s all just fine.”
There is a small number of non-believers in AA who think the literature is fine. These strange creatures largely hang their hats on a single line: “When, therefore, we speak to you of God, we mean your own conception of God.” (p. 47)
They put on blinders to what comes next, not even a paragraph later: “At the start this was all we needed to commence spiritual growth… Afterward, we found ourselves accepting many things which then seemed entirely out of reach... we had to begin somewhere.”
In a less kindly view, the clever subterfuge might be viewed as a “bait and switch.” The customer is “baited” by an attractive, advertised product that is unavailable. The customer is “baited” by an attractive, advertised product that is unavailable. Drawn to the store by the dishonest marketing of an unscrupulous retailer, prospective buyers are pressured by salespeople to consider higher priced items. In the world of commerce, consumer protection laws have criminalized the bait and switch. In the world of recovery, the little fraud is seen as helpful.
“But there is One who has all power – that One is God. May you find Him now!” (p. 59) Jeez! Why not just say that in the first place? Well at least we get to choose our own conception of God, right? … Right? … “Great Out Doors maybe?” No?
HEY!!! What happened to “Group of Drunks” and “Good Orderly Direction?”
The somewhat grumpy Bob Smith had been more honest. “God is God, young man,” he had told Clarence Snyder in 1938. Bill Wilson took a different tack of “getting them into the pews.” The savages’ belligerent defiance would quickiy melt away in the presence of God’s miracles, it was presumed.
This article will be offensive to some and it could have been more so; the “bait and switch” analogy could have been given precedence. Wikipedia refers to that as “fraud.” Rigorous honesty only goes so far, I suppose.
Speaking of deceitfulness, the time has come to reveal a little trickery of our own. Bobby Beach is bob k., and bob k. is Bobby Beach.
Some of you freaken suspected that.
Bob K has been something of an activist in the secular AA community. He has been one of the most prolific contributors to the websites AA Agnostica and AA Beyond Belief. He co-founded Whitby Freethinkers in 2013 and has made some efforts to support those who have started other nonreligious AA groups. In 2015, AA Agnostica published bob’s Key Players in AA History, a book that continues to sell well. Coming soon are a few other books, including “The Secret Diaries of Bill W.”
Articles by Bob K on AA Agnostica (those by Bobby Beach have a check mark – ):
Four-winged Microraptor, perhaps one of the earliest flying dinosaurs, may have molted just a bit at a time — similar to modern songbirds, Carolyn Gramling reported in “This dinosaur may have shed its feathers like modern songbirds” (SN: 8/15/20, p. 12).
Reader Jan Voelker asked if the dinosaur may somehow be related to the pileated woodpecker.
It’s hard to say just how closely related Microraptor might have been to woodpecker ancestors, Gramling says. Woodpeckers, along with toucans and honeyguides, belong to a biological order called Piciformes. “The evolutionary origins of the Piciformes are still quite murky,” she says. “There just isn’t a whole lot in the fossil record about their ancestors, although there are fossils of modern-looking Piciformes dating as far back as the Oligocene Epoch, which spanned 33.9 million to 23 million years ago.” But Piciformes are members of Aves, the biological class that includes all modern birds and that evolved from small feathered dinosaurs living during the Mesozoic Era, 252 million to 66 million years ago. Microraptor, which lived some 120 million years ago alongside ancient birds, is distantly related to Aves.
Reader Bob Garfield wondered how the image was made. “Is this a composite of a complete, 360-degree image of the sky or is the device looking in one general direction?” Garfield asked.
It’s a composite image of the entire sky, Temming says. “The telescope rotates continually to look at each point in the sky for 150 to 200 seconds on average and then moves on. Scientists stretch out the spherical view of the whole sky into this distended, ellipse-type shape so you can see it all at once on a 2-D surface,” she says.
Old dog, new math
A new formula for converting a dog’s age into human years is based on a comparative study of biological aging in Labrador retrievers and people, Bethany Brookshire reported in “Calculating a dog’s age in human years is harder than you think” (SN: 8/15/20, p. 5).
Reader Sue Jordan wondered how old her 13-year-old dog, a male black Lab and border collie mix, would be in human years according to the new equation.
“He’s around 72 years old in human years,” Brookshire says. “Keep in mind that the study doesn’t apply fully to all dogs, as it was done only in Labrador retrievers.” Collies and Labs might age at different rates. “As scientists do more of these comparisons, they will probably come up with different equations for different breeds,” she says.
“That 72 is a rough estimate; no one can say exactly how old your pup is in human years. But no matter what, I bet he’s great,” Brookshire says.
Reader Lou Puls wondered if the limitation on the rate at which the fundamental clock might tick could explain the arrow of time, or the idea that the total entropy (or disorder)
in the universe can only increase over time.
That’s a good question, Conover says. “When I interviewed physicist Martin Bojowald of Penn State for this study, I asked him the same thing. Sadly, he said that, at the moment, there’s no connection. It seems there’s no way to explain the arrow of time with this fundamental clock. At least, not yet,” she says.
When Nigerian physician Garba Iliyasu was 10, a venomous snake bit a family member. The man survived, but “it was quite severe,” Iliyasu recalls. “[He] was bleeding profusely.… From the nose. From the mouth. From the ear.”
Since then, Iliyasu, a specialist in infectious and tropical diseases, has tended to hundreds of snakebite victims at Kaltungo General Hospital, a health care hub for the surrounding Gombe State. During the two annual peaks in snakebite cases — the spring planting and autumn harvest seasons — “we see like six, seven to 10 patients in a day, on average,” he says. The hospital has only a few dozen beds. “Most times, you see patients on the floor.”
In the Western world, snakebites are a minor issue. In the United States and Europe, cases are rare and hardly ever fatal. Even in Australia — notorious for its deadly, venomous snakes — bites account for just a handful of annual deaths.
But in sub-Saharan Africa, about 270,000 people are bitten every year, resulting in more than 55,000 cases of post-traumatic stress disorder, over 14,700 amputations and about 12,300 deaths, Iliyasu and colleagues estimated in Toxicon in March 2019. Add in India and other snakebite hot spots and the annual numbers rise to more than 2 million bites that need clinical treatment, according to the World Health Organization. Between 80,000 and 138,000 victims die, and about three times that number have a life–changing disability.
Snakebites are “a neglected disease that affects the neglected section of the society,” Iliyasu says. The worst effects occur in mostly poor, rural communities that depend on farming and herding. Visit these places, he says, and “you will see how devastating the effect of snakebite is.” Victims are often the primary breadwinners of their households, so every death and disability contributes to the cycle of poverty.
2.7
million
Venomous snakebites per year estimated worldwide
But snakebites are finally getting the attention they’ve long needed. In 2017, the WHO officially recognized snakebites as a neglected tropical disease. That designation has led to an influx of funding for innovative research; the largest, more than $100 million, came in 2019 from the Wellcome Trust.
Effective snakebite treatments do exist, and those antivenoms are considered the “gold standard” of care. If a victim receives the right antivenom soon after a bite — within an hour or two — then the chances of survival are “very, very high,” says Nicholas Casewell, a biomedical scientist at the Liverpool School of Tropical Medicine in England.
But that “if” looms large, with big challenges remaining, including the difficulties of speedy access to care and the fact that most anti-venoms work against just a few of the hundreds of dangerous species of venomous snakes. Antivenoms are also “a technology that has seen limited innovation for 120 years,” says Andreas Laustsen, a biotech researcher and entrepreneur at the Technical University of Denmark in Kongens Lyngby.
Now, researchers from disparate fields of science are coming together to reimagine the way snakebites are managed. Casewell, Laustsen and others are tweaking current treatments, repurposing pharmaceuticals and even engineering toxin-stopping nanoparticles. The work offers hope that people everywhere, even in remote areas, will eventually be able to safely coexist with snakes.
Clear danger
Venomous snakebites, a neglected tropical disease, do the most damage in South and Southeast Asia, sub-Saharan Africa and parts of Central and South America. Recent data from India and Sub-Saharan Africa are still considered underestimates.
A tarnished gold standard
There’s a saying in snakebite care that “time is tissue.” The longer it takes to stop a snake’s venom from moving through the victim’s body, the more damage occurs. Destruction begins from the moment of a bite, and the cocktail of proteins and other molecules in the venom will continue to ravage until the immune system produces enough antibodies to remove or destroy those toxins. The problem is, by the time antibodies have ramped up, it’s often too late.
The tissue maxim is especially true for bites from vipers and other snakes with venoms that target the blood and soft tissues and thus tend to cause more physical damage. But speed is also important for bites from snakes with paralytic venoms, such as the Indian cobra (Naja naja) and southern Africa’s black mamba (Dendroaspis polylepi). Their nerve cell–targeting toxins will progressively slow muscles until the lungs and heart stop working.
That’s where antivenoms come in. They speed up the immune system’s clearance of toxins, because antivenoms are, themselves, antibodies pulled from the blood of large animals, usually horses, that have been injected with venom. When given soon after a snakebite, antivenoms work well.
But for myriad reasons, fast delivery often doesn’t happen.
In rural communities, there may be relatively few health care providers who can stock and administer the intravenously delivered drugs, which often require refrigeration. In India, for instance, the staff in rural public health clinics rarely have the resources or training to safely administer the drugs and monitor for treatment side effects.
Bit by a spitting cobra, this goat herder in Baringo County, Kenya, had to sell his herd to pay for treatment. Months later, the wound had not healed.N. Casewell
Patients are often sent several hours away to larger regional hospitals with more expertise. “A lot of [bite victims] die on the way,” says Kartik Sunagar, an evolutionary biologist at the Indian Institute of Science in Bangalore. Sunagar wrote about the challenges of developing antivenoms with Casewell, Laustsen and venom scientist Timothy Jackson of Liverpool in the August Trends in Pharmacological Sciences.
Once a patient arrives at a hospital, delays can still occur, Laustsen says, because medical staff wait until they’re completely sure someone needs antivenom before administering it. A large portion of snakebites are “dry,” which means no venom is injected, so antivenom isn’t always required.
Deciding which antivenom to use can be difficult. To glom on to and remove toxic substances, antibodies need to match their target almost exactly. And since each snake species makes its own unique blend of toxins, most venoms need a specific antivenom. Because bite victims can rarely reliably identify the species that bit them, doctors must wait for clear signs of damage to emerge to determine the right antivenom.
A “better safe than sorry” approach may seem warranted, but injecting antivenom when it’s not needed or if it’s the wrong kind can put the patient at even greater risk. As helpful as horse-derived antibodies can be, “the human immune system will recognize them as foreign,” Laustsen notes, and may launch an attack. This reaction to the antivenom itself can be life-threatening if not treated promptly.
A snakebite victim is in a coma and on dialysis to remove excess fluid and toxins from the blood. Medicshots/Alamy Stock Photo
Friendlier options
For the last decade or so, researchers have been working to take horses out of the equation to make antivenoms safer — and maybe more affordable. Laustsen is exploring a couple of approaches to avoiding the body’s reactions to horse-made antibodies.
One option is to produce “humanized” antibodies in the lab by replacing the ends of a human antibody gene with the venom-neutralizing parts from an effective equine antibody gene, so the patient’s body wouldn’t see the antibody proteins as foreign. But, even better, he hopes to discover effective fully human antibodies. With both approaches, he says, “you would remove at least 90 percent of all the side effects.”
Antivenom production currently relies on a century-old method: Snakes like these saw-scaled vipers are milked for venom, which is injected into horses and other animals. Neutralizing antibodies produced by the horses are then harvested for bite victims.Jeff Rotman/Alamy Stock Photo
Taking horses out of the mix may also open the door for designing antibodies that work against venoms from more than a few species. Laustsen and colleagues described one promising approach July 1 in Scientific Reports. The key is to take human antibody genes and insert them into bacteria-infecting viruses, which build the antibodies into their shells.
Since large databases of human antibody genes already exist, a whole variety of different human antibodies can be inserted into viruses for high-throughput testing to find antibodies that can bind to — and perhaps neutralize — venom toxins.
As a proof of concept, Laustsen’s team tested 40 billion antibodies from people, and identified one particularly exciting candidate: It protected human cells in lab dishes from more than a dozen lethal toxins from three cobra species.
Once the most broadly effective antibodies are found, Laustsen hopes to copy a page from the insulin-production handbook. For diabetes treatment, insulin used to be extracted from the pancreases of animals; now, it’s made by engineered bacteria in large fermentation tanks. A similar process could work to produce broad-spectrum antivenom, he says.
Moving antibody production out of animals could also have another important benefit: lower production costs. Right now, “antivenom is one of the most expensive drugs that you can find in the rural areas,” explains Muhammad Hamza, a medical doctor who, like Iliyasu, splits his time between research at Nigeria’s Aminu Kano Teaching Hospital and treating patients at the regional treatment center in Gombe State. Many of Hamza’s patients could be saved by antivenom, he says, but they can’t afford to pay for it. If the government hasn’t kept the clinic stocked with free medicine, patients die.
In Nigeria, a vial of antivenom costs around $60 to $70, Iliyasu says. He’s seen patients sell their animals, homes and farms to pay for treatment.
Antivenoms engineered without animals would save patients money because the ideal mix of antibodies would be more potent. At least 70 percent of the antibodies in current antivenoms don’t neutralize venom toxins at all, Iliyasu notes. As a result, it often takes several vials of antivenom — sometimes as many as 10 — to treat a bite patient. Boosting the percentage of neutralizing antibodies in each vial would go a long way toward making antivenoms affordable, Iliyasu says — and that’s why he’s excited to see the move away from animal-based production.
Mixed bag
Snake venoms often contain dozens to hundreds of individual toxins. Two snakes’ venom blends are shown here. The carpet viper’s venom is heavy on metalloproteinase toxins, which can cause paralysis and tissue damage.
Most snake venoms, which can vary greatly among snake species, fall into recognizable groups. Four of the most common and pernicious groups and their toxic effects are listed below.
• Immune system: Painful swelling • Blood: Blood vessel damage; bruising and bleeding, especially internal • Tissue: Skin blistering and visible wounds • Nervous sytem: Paralysis
Serine proteases
Cut up certain proteins
• Immune system: Mild, painful swelling • Blood: Bruising and bleeding, internal or external • Nervous sytem: Mild pain
Three-finger toxins
Block or activate other proteins
• Blood: Bruising and bleeding, internal and external • Tissue: Racing heart and cardiac arrest; visible wounds • Nervous system: Numbness; paralysis
Phospholipase A2s
Main molecular action: Cut up certain fats Potential effects on the body: • Immune system: Intense inflammation (redness and swelling) • Blood: Bruising and bleeding • Tissue: Muscle damage; kidney failure • Nervous system: Acute, intense pain; paralysis
Metalloproteinases
Main molecular action: Cut up certain proteins Potential effects on the body: • Immune system: Painful swelling • Blood: Blood vessel damage; bruising and bleeding, especially internal • Tissue: Skin blistering and visible wounds • Nervous system: Paralysis
Serine proteases
Main molecular action: Cut up certain proteins Potential effects on the body: • Immune system: Mild, painful swelling • Blood: Bruising and bleeding, internal or external • Nervous system: Mild pain
Three-finger toxins
Main molecular action: Block or activate other proteins Potential effects on the body: • Blood: Bruising and bleeding, internal and external • Tissue: Racing heart and cardiac arrest; visible wounds • Nervous system: Numbness; paralysis
Sources: L.-O. Albulescu et al/BioRxiv.org 2020; C.R. Ferraz et al/Frontiers in Ecology and Evolution 2019
A pill for snakebite
Other researchers are turning to existing drugs to expand options for snakebite treatments.
Venom toxins generally cause harm by performing specific molecular actions, such as cutting up certain proteins or fats within cells. Targeted molecules that interfere with that nefarious work could potentially stop the toxins.
The idea of using drugs other than antibodies to inhibit venom toxins isn’t new. But it wasn’t until the molecular and genetic technology revolutions of the late 20th century that scientists could really deconstruct venoms to figure out which components are responsible for a venom’s worst effects. “We now have a very good handle on what the toxins are,” Casewell says.
It’s unlikely that one drug, or even a combination, would be able to neutralize the diversity of harmful toxins present in snake venoms and work as effectively as traditional antivenoms. But Casewell’s aim isn’t to replace antivenoms; he wants to safely slow down the most pernicious venom toxins to buy patients time to get to a clinic.
He and colleagues have so far focused on metalloproteinases — toxins that chop up proteins and are major players in the lethal and destructive nature of tissue-destroying venoms, such as those in saw-scaled vipers (Echis spp.). Casewell’s group picked a few drugs already on the market that bind up the metal ions that these proteinases need to function, and right off the bat, the drugs were surprisingly successful.
The group demonstrated that an existing small molecule drug used to treat heavy metal poisoning could reduce the deadly damage of viper bites in lab animals (SN: 6/6/20, p. 12). And when paired with another drug that inhibits a family of toxins that chew up certain fats, the drug was even more powerful. In animal tests, the combination neutralized the venoms of a more diverse collection of five snake species from all over the world.
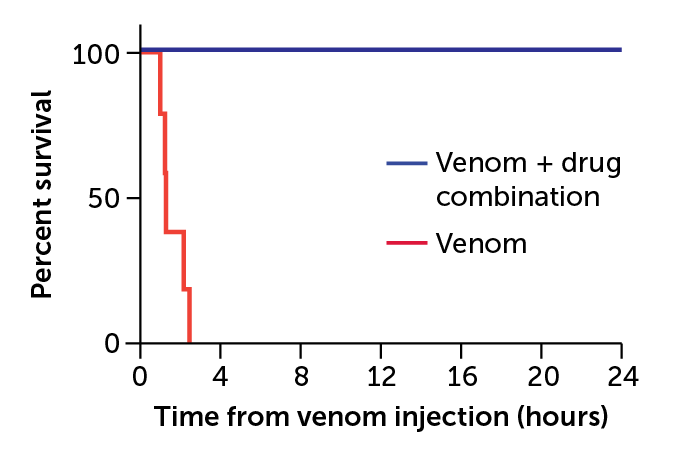
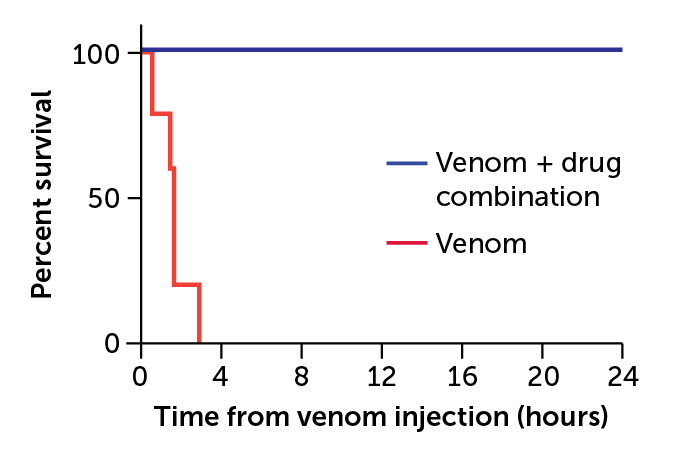
Drug duo
Two drugs together — the PLA2 inhibitor varespladib, and the metalloproteinase inhibitor marimastat — saved mice from lethal doses of five different snake venoms (results against two of the venoms shown below). Even when the drugs were given 15 minutes after the venom injection, the mice lived (blue lines). Mice that didn’t get the drugs died within four hours (red).
Effect of two-drug combination in mice injected with snake venom
The work is “quite exciting,” Casewell says, because it means small molecule drugs might be able to overcome the problem of geographic fragmentation — each venom needs its own antidote — that keeps antivenom markets too small and nonlucrative for pharmaceutical companies to invest in.
As a bonus, such small molecules are available in pill form and don’t need refrigeration or expert administration, making them easier to distribute in rural communities. In that way, such drugs could become an important “bridge to care,” Iliyasu says.
Next generation of treatments
While pills alone may never be a stand-alone treatment for snakebites, there are other alternatives to conventional antivenoms, says Shih-Hui Lee of the University of California, Irvine. “We can use a polymer.”
Lee and colleague Kenneth Shea are new to the field of snakebite treatment. “We’re not snake venom people,” Shea admits. They’re not even biologists. The two are materials scientists. But their approach to overhauling antivenom is so out of the box that it’s getting noticed.
Both spent much of their careers designing carbon polymers — essentially, plastic nanoparticles — with specific, desirable properties. After a while, the duo started to wonder if their designer plastics, which could bind to certain parts of proteins, could mimic the actions of antibodies.
Shea started with melittin, a bee venom toxin. To his surprise, the polymer nanoparticles worked. When injected into mice shortly after the injection of a life-threatening dose of melittin, the particles bound up enough of the toxin to save the animals’ lives, Shea and colleagues reported in the Journal of the American Chemical Society in 2010.
Those results helped him recruit Lee to the antivenom project and convince well-respected snakebite expert José María Gutiérrez of the University of Costa Rica in San José to collaborate. With his help, Shea and Lee set their sights on phospholipase A2s, a large family of toxins found in many deadly snake venoms.
Once again, Lee says, the polymer nanoparticles neutralized the toxins. In 2018, the particles proved effective against another family of snake toxins called three-finger toxins. The “plastic” antibodies saved mice from cobra venom, and healthy mice that received them had no adverse reactions, the team reported in PLOS Neglected Tropical Diseases.
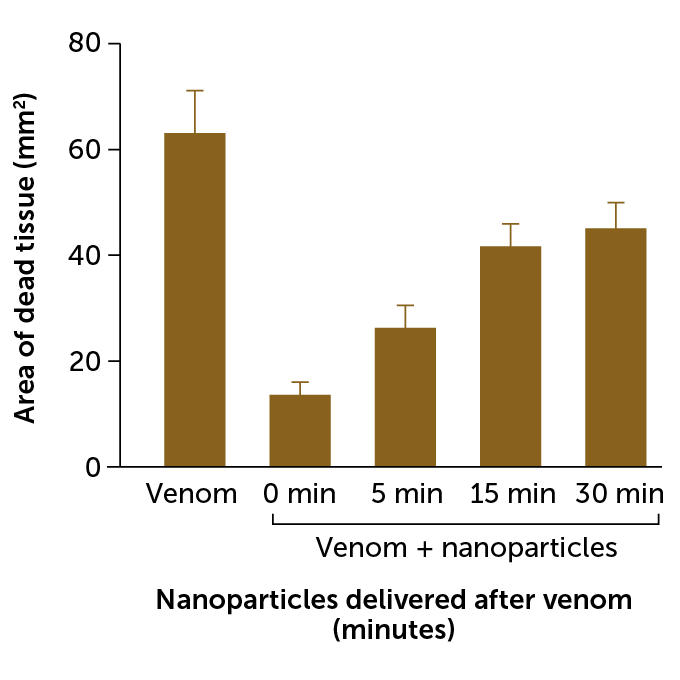
Cobra combat
When tested in mice, synthetic nanoparticle antibodies prevented skin tissue death caused by black-necked spitting cobra venom. The nanoparticles were most effective when injected into the wound right after the venom was injected (0 min); the longer the wait, the larger the wound.
Source: J. O’Brien et al/PLOS Neglected Tropical Diseases 2018
There are still some design challenges to overcome before testing the polymers in people. The team wants to put these synthetic antibodies into injectable devices — much like an EpiPen — but right now, the nanoparticles are probably too big. So the next hurdle is to make them smaller and more able to travel from the injection site in a muscle to the surrounding tissues.
But the biggest challenge is convincing funding agencies that synthetic antibodies should be on the table. The hesitancy is understandable, Shea says, as there’s nothing like these nanoparticles on the market. “This is untested, so there has to be an element of faith in this,” he says.
Still, Shea and Lee believe in their creation. Producing a broad-spectrum antivenom with the nanoparticles “is technically much less challenging” than with biological antibodies, Shea says, so if the team can secure investors, he thinks the nanoparticles have the potential to be “a quite cheap antidote.”
Others are stepping out of the box, as well. Thanks to the influx of funding in the last few years, researchers around the world are trying all sorts of unconventional approaches to snakebite remedies. There are labs hoping to design DNA molecules known as aptamers that act like antibodies. Others are turning to animals, such as opossums, that are naturally immune to venoms in the hopes of translating that immunity into new drugs. All of this work is leading to some truly exciting technological developments, Casewell says.
But none of it will matter if there aren’t also investments in infrastructure and education, Hamza warns. “It is one thing to have the drug.… It’s another thing to get it available to the remotest parts of the world.”
He’s more excited about smartphone apps that could tell people in remote areas where the closest available antivenom is, for instance. And something as simple as providing farmers solid boots with instructions on when and why to wear them could prevent countless snakebites from happening in the first place.
With millions of snakebites occurring every year, there’s certainly many opportunities to improve the situation — and all of them need attention, Casewell says. That attention is finally coming. “This is kind of a once-in-a-lifetime moment for snakebites,” he says.
Tommy Piluyev, a 24 years old man is filing a lawsuit against Starbucks, the international coffee giant as a defect in their cups reportedly burnt this man’s genitals. The guy ordered hot tea at Starbucks which had a temperature of almost 100C but this tea was spilled due to the defect in the cap while he was sitting in his car. This incident took place in Roseville, California, making him suffer second-grade burns.
Tommy picked a take away order and while he was receiving his ordered tea, a sufficient amount of the tea leaked on his body while he was still seated in the car. His lawsuit explains the tremendous intensity of pain that he suffered that he eventually chooses to park his car nearby, take off his trousers, and see how the tea has burnt his genitals.
He calls this experience excruciating as getting naked and sex is extremely awkward and somehow painful for him after this incidence. The skin discoloration caused by the tea spill has affected his genitals as well as thighs, affecting his confidence.
The father of one is a resident of California who was immediately rushed to a hospital for the burns. The lawyers report that he had to spend 11 days in the hospital for getting his burns treated, learning to function normally.
This incident took place two years ago back in October 2018. Piluyev and his wife Liudmila Maftey are together in this lawsuit against Starbucks as well as the cup making company named “Pactiv Packaging” for the negligence charges along with the product liability charges.
Piluyev ordered two grande of the honey citrus mint teas from the Starbucks drive-thru located in the Roseville near Sacramento.
The lawsuit says that Piluyev experienced severe burnt injuries after the lid almost missed its seal and dislodged from the cup. The tea was directly spilled on the hand of the Piluyev and burnt his hands, belly, and pelvis.
While his car was still in the drive-thru it wasn’t possible for him to rush out of the car so he rushed the car and stopped by the nearest parking lot. The hospital where he went for getting the emergency care for blisters that showed up on his stomach, penis, thighs, scrotum, and peritoneum.
There are photos of him admitted to the hospital while receiving the treatment for the burnt wounds.
The lawsuit explains Piluyev to be suffering from the intravenous pain along with huge blisters that require intensive care. His condition made him dependent upon other people even for the smallest things including the personal grooming and cleaning as he was even unable to move his fingers.
After he was discharged from the hospital, his wife was taking care of him for five months, after which he was finally able to walk and take care of himself. Piluyev reports that his condition has made sex extremely painful for him and he doesn’t even feel confident about himself. He is also not able to do other things that he once enjoyed especially playing the piano after getting these second-degree burns.
Sen. Cory Gardner, a Republican running in a tight race for reelection in Colorado, says he wants to protect people with medical conditions.
In a mid-September tweet released by his campaign, he promoted legislation he introduced in August that he says will do just that.
“People like my mother who battle chronic diseases are heroes,” read the tweet. “I authored the bill to guarantee coverage to people with pre-existing conditions — no matter what happens to Obamacare — because some things matter more than politics.”
Gardner has voted repeatedly to repeal the Affordable Care Act, the first federal law to guarantee people with health problems that they could buy insurance when shopping for their own coverage — at the same cost as for healthier consumers.
Polls show broad public support for keeping the ACA’s preexisting condition protections, while also indicating a consistent, if narrow, majority favoring the overall law.
The popularity of those protections has led Gardner, as well as other GOP candidates facing tough challengers, to swear their allegiance to protecting people with medical conditions, despite their records. In previous fact checks, we found Sen. Martha McSally’s promise always to protect preexisting conditions to be False. President Donald Trump also has made related statements, which have ranged from False to Pants on Fire.
That got us thinking: Would Gardner’s legislation, dubbed “The Pre-Existing Conditions Protection Act,” actually guarantee these protections if the ACA didn’t exist? We decided to investigate.
The bill, which was introduced in August, and has no co-sponsors. It’s very short, only 117 words in total.
The main section is a single very long sentence: “A group health plan and a health insurance issuer offering group or individual health insurance coverage may not impose any pre-existing condition exclusion with respect to such plan or coverage, factor health status into premiums or charges, exclude benefits relating to pre-existing conditions from coverage, or otherwise exclude benefits, set limits, or increase charges based on any pre-existing condition or health status.”
We reached out to the Gardner campaign to ask for more information.
A campaign spokesperson reiterated in an email that Gardner’s goal is “to guarantee coverage for individuals with preexisting conditions and ensure they cannot be charged more as a result of their underlying medical conditions.”
Thomas Miller, a resident fellow at the American Enterprise Institute, a think tank in Washington, D.C., quipped that the main goal might be something else entirely.
“It’s probably about 100 words too long,” Miller said. “It could have said, ‘I’m running for election. I’ll do whatever is necessary.’”
Past Votes, Present Messages
Proponents of the ACA emphasized that the law would help people with medical conditions as they worked to get it passed by Congress, which happened in 2010 following a yearlong failed effort by Democrats to win Republican support. Among a host of other provisions, the law bars insurers from rejecting applicants with medical conditions, as they routinely did when considering individual applicants before the law passed. Nor can insurers charge the sick more than the healthy.
Since the law went into effect in 2014, it has faced many efforts by Republicans in Congress, including Gardner, to repeal it.
It has also faced three Supreme Court challenges. It survived the first two, although one ruling allowed states to opt out of its expansion of Medicaid programs for the poor. The still-pending case was first brought in 2018 by 20 states and is supported by the Trump administration. That case could overturn the entire law, although the court won’t hear arguments on the issue before the election. And that brings us back to Gardner’s bill. An obvious difference between that proposal and the ACA is length. Gardner’s bill is one page, while the ACA runs to several hundred.
And Gardner’s claim seems pegged to the legislative language that says insurers can’t impose a “pre-existing condition exclusion,” which sounds fairly straightforward.
But it’s not, experts say.
“It’s an adorable little bill but does not address any of the main issues,” said Linda Blumberg, a fellow at the nonprofit Urban Institute’s Health Policy Center. “You need a package of policies working together in order to create real protections for people to have coverage to meet their health care needs.”
For instance, the bill does not explicitly bar insurers from outright rejecting applicants with medical conditions, something known as “guaranteed issue.”
“‘Guaranteed issue’ is not in the language of the bill,” said Miller at AEI.
Instead, the language may simply prohibit insurers from restricting services related to a medical condition only if they choose to sell an individual insurance in the first place, he said.
Compare that with the ACA, which says every insurer selling individual or group coverage “must accept every employer and individual in the State that applies.”
Also needed in legislation aiming to protect people with medical problems, said Blumberg, are provisions for subsidies to help people of low and moderate income afford their premiums. The ACA has those, along with specific enrollment periods, so that people don’t wait until they are sick to sign up. Without them, mainly those with medical conditions might sign up, driving up costs and premiums. That, in turn, can price people, especially the sick, out of future coverage.
Another way Gardner’s bill differs from the ACA is that it does not list benefits that must be included in a health insurance policy. The ACA requires insurers to cover 10 broad categories of care, including hospitalization, prescription drugs, childbirth, substance abuse treatment and mental health care.
“Without that, insurers could sell products that don’t cover very much, which is what we had prior to 2014,” Blumberg added, which is one way to discourage those who are sick from even applying. “It was difficult to find a product that covered prescription drugs, and we even saw policies that didn’t cover chemotherapy.”
So, What About Costs?
Gardner’s legislation says insurers can’t “factor health status into premiums or charges.”
So insurers could not charge people more simply because they have diabetes, say, or cancer. Still, that leaves open a whole lot of other things that insurers could consider when setting premiums for individuals, such as such as gender or occupation, which could stand in as a proxy for health. Unlike the ACA, it does not bar insurers from setting annual or lifetime dollar limits on coverage, which could disproportionately affect people with costly medical conditions.
The ACA allows insurers to vary premiums for only three reasons: where people live, their age and whether they use tobacco. It sets upper limits, such as charging older folks no more than three times what younger enrollees pay.
Douglas Holtz-Eakin, president of the American Action Forum, who wrote a blog post cited by the Gardner campaign, said the proposed legislation is a starting point — a place holder, if you will. His piece mentioned it near the end of a broader look at the Trump administration’s health platform going into the election.
Responding to questions about Gardner’s legislation, Holtz-Eakin said that if the ACA were to be struck down, Gardner would likely add provisions to it.
“I don’t think it’s intended to be a replacement bill but a provision to make sure people can get coverage,” said Holtz-Eakin. “It’s quite clear on the aim to ensure that people with pre-existing conditions can get insurance, but it doesn’t address every single policy issue that’s out there.”
Health law professor Mark Hall at Wake Forest University said Gardner’s legislation could survive if the ACA were struck down by the Supreme Court, but he noted that Congress would be unlikely to adopt the Gardner bill as written.
“A freestanding protection of pre-existing conditions without any supporting provisions to keep insurance affordable or encourage people to purchase it before they become sick, is almost certain to cause serious harms to the market,” Hall wrote in an email. “Therefore, a lot more is needed to overcome legitimate objections that almost certainly will be made from both sides of the political aisle.”
Our Ruling
Because protecting people with medical conditions requires many moving parts, the brevity of Gardner’s proposal makes it appear to be a fig leaf for a political problem rather than a means to guarantee protections for people with preexisting conditions.
The legislation is unclear on whether it guarantees that people with health problems will be able to buy insurance in the first place. And, even if they can, they may well find it priced out of reach because the legislation does not bar insurers from varying premiums widely on the basis of age, gender or occupation.
Viewed in its most favorable light, Gardner’s 117-word proposal would only serve as a place holder for larger legislation, upon which more protections would have to be layered to bolster the effectiveness of its guarantee.
SEELEY LAKE, Mont. — When researchers arrived in this town tucked in the Northern Rockies three years ago, they could still smell the smoke a day after it cleared from devastating wildfires. Their plan was to chart how long it took for people to recover from living for seven weeks surrounded by relentless smoke.
They still don’t know, because most residents haven’t recovered. In fact, they’ve gotten worse.
Forest fires had funneled hazardous air into Seeley Lake, a town of fewer than 2,000 people, for 49 days. The air quality was so bad that on some days the monitoring stations couldn’t measure the extent of the pollution. The intensity of the smoke and the length of time residents had been trapped in it were unprecedented, prompting county officials to issue their first evacuation orders due to smoke, not fire risk.
Many people stayed. That made Seeley Lake an ideal place to track the long-term health of people inundated by wildfire pollution.
So far, researchers have found that people’s lung capacity declined in the first two years after the smoke cleared. Chris Migliaccio, an immunologist with the University of Montana, and his team found the percentage of residents whose lung function sank below normal thresholds more than doubled in the first year after the fire and remained low a year after that.
“There’s something wrong there,” Migliaccio said.
While it’s long been known that smoke can be dangerous when in the thick of it — triggering asthma attacks, cardiac arrests, hospitalizations and more — the Seeley Lake research confirmed what public health experts feared: Wildfire haze can have consequences long after it’s gone.
That doesn’t bode well for the 78 million people in the western United States now confronting historic wildfires.
Toxic air from fires has blanketed California and the Pacific Northwest for weeks now, causing some of the world’s worst air quality. California fires have burned roughly 2.3 million acres so far this year, and the wildfire season isn’t over yet. Oregon estimates 500,000 people in the state have been under a notice to either prepare to evacuate or leave. Smoke from the West Coast blazes has drifted as far away as Europe.
Extreme wildfires are predicted to become a regular occurrence due to climate change. And, as more people increasingly settle in fire-prone places, the risks increase. That’s shifted wildfires from being a perennial reality for rural mountain towns to becoming an annual threat for areas across the West.
Dr. Perry Hystad, an associate professor in the College of Health and Human Sciences at Oregon State University, said the Seeley Lake research offers unique insights into wildfire smoke’s impact, which until recently had largely been unexplored. He said similar studies are likely to follow because of this fire season.
“This is the question that everybody is asking,” Hystad said. “‘I’ve been sitting in smoke for two weeks, how concerned should I be?’”
Migliaccio wants to know whether the lung damage he saw in Seeley Lake is reversible — or even treatable. (Think of an inhaler for asthma or other medication that prevents swollen airways.)
But those discoveries will have to wait. The team hasn’t been able to return to Seeley Lake this year because of the coronavirus pandemic.
Migliaccio said more research is needed on whether wildfire smoke damages organs besides the lungs, and whether routine exposure makes people more susceptible to diseases.
“Now you have the combination of flu season and COVID and the wildfires,” Migliaccio said. “How are all these things going to interact come late fall or winter?”
A Case Study
Seeley Lake has long known smoke. It sits in a narrow valley between vast stretches of thick forests.
On a recent September day, Boyd Gossard stood on his back porch and pointed toward the mountains that were ablaze in 2017.
Gossard, 80, expects to have some summer days veiled in haze. But that year, he said, he could hardly see his neighbor’s house a few hundred feet away.
“I’ve seen a lot of smoke in my career,” said Gossard, who worked in timber management and served as a wildland firefighter. “But having to just live in it like this was very different. It got to you after a while.”
When Missoula County health officials urged people to leave town and flee the hazardous smoke, many residents stayed close to home. Some said their jobs wouldn’t let them leave. Others didn’t have a place to go — or the money to get there.
Health officials warned those who stayed to avoid exercising and breathing too hard, to remain inside and to follow steps to make their homes as smoke-free as possible. The health department also worked to get air filters to those who needed them most.
But when flames got too close, some people had to sleep outside in campsites on the other side of town.
Understanding the Science of Smoke
One of the known dangers of smoke is particulate matter. Smaller than the width of a human hair, it can bypass a body’s defenses, lodging deep into lungs. Lu Hu, an atmospheric chemist with the University of Montana, said air quality reports are based on how much of that pollution is in the air.
“It’s like lead; there’s no safe level, but still we have a safety measure for what’s allowable,” Hu said. “Some things kill you fast and some things kill you slowly.”
While air quality measurements can gauge the overall amount of pollution, they can’t assess which specific toxins people are inhaling. Hu is collaborating with other scientists to better predict how smoke travels and what pollutants people actually breathe.
He said smoke’s chemistry changes based on how far it travels and what’s burning, among other factors.
Over the past few years, teams of researchers drove trucks along fire lines to collect smoke samples. Other scientists boarded cargo planes and flew into smoke plumes to take samples right from a fire’s source. Still others stationed at a mountain lookout captured smoke drifting in from nearby fires. And ground-level machines at a Missoula site logged data over two summers.
Bob Yokelson, a longtime smoke researcher with the University of Montana, said scientists are getting closer to understanding its contents. And, he said, “it’s not all bad news.”
Temperature and sunlight can change some pollutants over time. Some dangerous particles seem to disappear. But others, such as ozone, can increase as smoke ages.
Yokelson said scientists are still a long way from determining a safe level of exposure to the 100-odd pollutants in smoke.
“We can complete the circle by measuring not only what’s in smoke, but measuring what’s happening to the people who breathe it,” Yokelson said. “That’s where the future of health research on smoke is going to go.”
Coping With Nowhere to Flee
In the meantime, those studying wildland smoke hope what they’ve learned so far can better prepare people to live in the haze when evacuation isn’t an option.
Joan Wollan, 82, was one of the Seeley Lake study participants. She stayed put during the 2017 fire because her house at the time sat on a border of the evacuation zone.
The air made her eyes burn and her husband cough. She ordered air filters to create cleaner air inside her home, which helped.
On a recent day, the air in Wollan’s new neighborhood in Missoula turned that familiar gray-orange as traces of fires from elsewhere appeared. Local health officials warned that western Montana could get hit by some of the worst air quality the state had seen since those 2017 fires.
If it got bad enough, Wollan said, she’d get the filters out of storage or look for a way to get to cleaner air — “if there is someplace in Montana that isn’t smoky.”
KHN senior correspondent Liz Szabo discussed COVID-19 vaccines on Newsy’s “Morning Rush” on Tuesday and on iHeartRadio’s “The Daily Dive” on Wednesday.
KHN Midwest correspondent Lauren Weber spoke to Margie Shafer on KCBS Radio in San Francisco on Wednesday about how more than 20 states aren’t fully counting COVID-19 antigen tests.
Bernard J. Wolfson, columnist and senior correspondent for California Healthline, discussed masking up for both COVID-19 and smoke from wildfires on Newsy’s “Morning Rush” on Thursday.
Over the objections of drugmakers, the Trump administration is expected within weeks to finalize its plan that would allow states to import some prescription medicines from Canada.
Six states — Colorado, Florida, Maine, New Hampshire, New Mexico and Vermont — have passed laws allowing them to seek federal approval to buy drugs from Canada to give their residents access to lower-cost medicines.
But industry observers say the drug importation proposal under review by the administration is squarely aimed at Florida — the most populous swing state in the November election. Trump’s support of the idea initially came at the urging of Florida Gov. Ron DeSantis, a close Republican ally.
The DeSantis administration is so confident Trump will move ahead with allowing drug importation that it put out a request June 30 for private companies to bid on a three-year, $30 million contract to run the program. It hopes to award the contract in December.
Industry experts say Florida is likely to be the first state to win federal approval for a drug importation plan — something that could occur before the November election.
“Approving Florida would feel like the politically astute thing to do,” said Mara Baer, a Colorado-based health consultant who has worked with Florida on its importation proposal.
Ben England, CEO of FDAImports, a consulting firm in Glen Burnie, Maryland, said the OMB typically has 60 days to review final rules, although he expects this one could be completed before Nov. 3 and predicted there’s a small chance it could get finalized and Florida’s request approved by then. “It’s an election year, so I do see the current administration trying to use this as a talking point to say ‘Look what we’ve accomplished,’” he said.
Florida also makes sense because of the large number of retirees, who face high costs for medicines despite Medicare drug coverage.
The DeSantis administration did not respond to requests for comment.
Trump boasted about his importation plan during an October speech in The Villages, a large retirement community about 60 miles northwest of Orlando. “We will soon allow the safe and legal importation of prescription drugs from other countries, including the country of Canada, where, believe it or not, they pay much less money for the exact same drug,” Trump said, with DeSantis in attendance. “Stand up, Ron. Boy, he wants this so badly.”
The Food and Drug Administration released a detailed proposal last December and sought comments. A final plan was delivered Sept. 10 to the Office of Management and Budget for review, signaling it could be unveiled within weeks.
The proposal would regulate how states set up their own programs for importing drugs from Canada.
Prices are cheaper because Canada limits how much drugmakers can charge for medicines. The United States lets free markets dictate drug prices.
The pharmaceutical industry signaled it will likely sue the Trump administration if it goes forward with its importation plans, saying the plan violates several federal laws and the U.S. Constitution.
But the most stinging rebuke of the Trump importation plan came from the Canadian government, which said the proposal would make it harder for Canadian citizens to get drugs, putting their health at risk.
“Canada will employ all necessary measures to safeguard access for Canadians to needed drugs,” the Canadian government wrote in a letter to the FDA about the draft proposal. “The Canadian drug market and manufacturing capacity are too small to meet the demand of both Canadian and American consumers for prescription drugs.”
Without buy-in from Canada, any plan to import medicines is unlikely to succeed, officials said.
Ena Backus, director of Health Care Reform in Vermont, who has worked on setting up an importation program there, said states will need help from Canada. “Our state importation program relies on a willing partner in Canada,” she said.
For decades, Americans have been buying drugs from Canada for personal use — either by driving over the border, ordering medication on the internet or using storefronts that connect them to foreign pharmacies. Though illegal, the FDA has generally permitted purchases for individual use.
The practice has been popular in Florida. More than a dozen storefronts across the state help consumers connect to pharmacies in Canada and other countries. Several cities, state and school districts in Florida help employees get drugs from Canada.
The administration’s proposal builds on a 2000 law that opened the door to allowing drug importation from Canada. But that provision could take effect only if the Health and Human Services secretary certified importation as safe, something that Democratic and Republican administrations have refused to do.
The drug industry for years has said allowing drugs to be imported from Canada would disrupt the nation’s supply chain and make it easier for unsafe or counterfeit medications to enter the market.
Trump, who made lowering prescription drug prices a signature promise in his 2016 campaign, has been eager to fulfill his pledge. In July 2019, at Trump’s direction, HHS Secretary Alex Azar said the federal government was “open for business” on drug importation, a year after calling drug importation a “gimmick.”
The administration envisions a system in which a Canadian-licensed wholesaler buys directly from a manufacturer for drugs approved for sale in Canada and exports the drugs to a U.S. wholesaler/importer under contract to a state.
Florida’s legislation — approved in 2019 — would set up two importation programs. The first would focus on getting drugs for state programs such as Medicaid, the Department of Corrections and county health departments. State officials said they expect the programs would save the state about $150 million annually.
The second program would be geared to the broader state population.
In response to the draft rule, the states seeking to start a drug importation program suggested changes to the administration’s proposal.
“Should the final rule not address these areas of concern, Colorado will struggle to find appropriate partners and realize significant savings for consumers,” Kim Bimestefer, executive director of the Colorado Department of Health Care Policy & Financing, told the FDA in March.
Among the state’s concerns is that it would be limited to using only one Canadian wholesaler, and without competition the state fears prices might not be as low as officials hoped. Bimestefer also noted that under the draft rule, the federal government would approve the importation program for only two years and states need a longer time frame to get buy-in from wholesalers and other partners.
Colorado officials estimate importing drugs from Canada could cut prices by 54% for cancer drugs and 75% for cardiac medicines. The state also noted the diabetes drug Jardiance costs $400 a month in the United States and sells for $85 in Canada.
Several states worry some of the most expensive drugs — including injectable and biologic medicines — were exempt from the federal rule. Those drug classes are not allowed to be imported under the 2000 law.
However, in an executive order in July, Trump said he would allow insulin to be imported if Azar determined it is required for emergency medical care. An HHS spokesman would not say whether Azar has done that.
Jane Horvath, a health policy consultant in College Park, Maryland, said the administration faces several challenges getting an importation program up and running, including possible opposition from the pharmaceutical industry and limits on classes of drugs that can be sold over the border.
“Despite the barriers, the programs are still quite worthwhile to pursue,” she said.
Maine’s top health official said the administration should work with the Canadian government to address Canada’s concerns. HHS officials refused to say whether such discussions have started.
Officials in Vermont, where the program would also include consumers covered by private insurance, remain hopeful.
“Given that we want to reduce the burden of health care costs on residents in our state, then it is important to pursue this option if there is a clear pathway forward,” Backus said.
Older adults are asking this question anew in light of the ongoing toll of the coronavirus pandemic — disrupted lives, social isolation, mounting deaths. Many are changing their minds.
Some people who planned to move to senior housing are now choosing to live independently rather than communally. Others wonder whether transferring to a setting where they can get more assistance might be the right call.
These decisions, hard enough during ordinary times, are now fraught with uncertainty as the economy falters and COVID-19 deaths climb, including tens of thousands in nursing homes and assisted living centers.
Teresa Ignacio Gonzalvo and her husband, Jaime, both 68, chose to build a house rather than move into a continuing care retirement community when they relocate from Virginia Beach, Virginia, to Indianapolis later this year to be closer to their daughters.
Having heard about lockdowns around the country because of the coronavirus, Gonzalvo said, “We’ve realized we’re not ready to lose our independence.”
Alissa Ballot, 64, is planning to leave her 750-square-foot apartment in downtown Chicago and put down roots in a multigenerational cohousing community where neighbors typically share dining and recreation areas and often help one another.
“What I’ve learned during this pandemic is that personal relationships matter most to me, not place,” she said.
Kim Beckman, 64, and her husband, Mike, were ready to give up being homeowners in Victoria, Texas, and join a 55-plus community or rent in an independent living apartment building in northern Texas before COVID-19 hit.
Now, they’re considering buying an even bigger home because “if you’re going to be in the house all the time, you might as well be comfortable,” Beckman said.
“Everyone I know is talking about this,” said Wendl Kornfeld, 71, who lives on the Upper West Side of Manhattan. She has temporarily tabled the prospect of moving into a continuing care retirement community being built in the Bronx.
“My husband and I are going to play it by ear; we want to see how things play out” with the pandemic, she said.
In Kornfeld’s circles, people are more committed than ever to staying in their homes or apartments as long as possible — at least at the moment. Their fear: If they move to a senior living community, they might be more likely to encounter a COVID outbreak.
“All of us have heard about the huge number of deaths in senior facilities,” Kornfeld said. But people who stay in their own homes may have trouble finding affordable help there when needed, she acknowledged.
More than 70,000 residents and staff members in nursing homes and assisted living facilities had died of COVID-19 by mid-August, according to the latest count from KFF (Kaiser Family Foundation). This is an undercount because less than half of states are reporting data for COVID-19 in assisted living. Nor is data reported for people living independently in senior housing. (KHN is an editorially independent program of KFF.)
Nervousness about senior living has spread as a result, and in July, the National Investment Center for Seniors Housing & Care reported the lowest occupancy rates since the research organization started tracking data 14 years ago. Occupancy dropped more in assisted living (a 3.2% decline from April through June, compared with January through March) than in independent living (a 2.4% decline). The organization doesn’t compile data on nursing homes.
The potential for social isolation is especially worrisome, as facilities retain restrictions on family visits and on group dining and activities. (While states have started to allow visits outside at nursing homes and assisted living centers, most facilities don’t yet allow visits inside — a situation that will increase frustration when the weather turns cold.)
Beth Burnham Mace, NIC’s chief economist and director of outreach, emphasized that operators have responded aggressively by instituting new safety and sanitation protocols, moving programming online, helping residents procure groceries and other essential supplies, and communicating regularly about COVID-19, both on-site and in the community at large, much more regularly.
Mary Kazlusky, 76, resides in independent living at Heron’s Key, a continuing care retirement community in Gig Harbor, Washington, which is doing all this and more with a sister facility, Emerald Heights in Redmond, Washington.
“We all feel safe here,” she said. “Even though we’re strongly advised not to go into each other’s apartments, at least we can see each other in the hall and down in the lobby and down on the decks outside. As far as isolation, you’re isolating here with over 200 people: There’s somebody always around.”
One staff member at Heron’s Key tested positive for COVID-19 in August but has recovered. Twenty residents and staff members tested positive at Emerald Heights. Two residents and one staff member died.
Colin Milner, chief executive officer of the International Council on Active Aging, stresses that some communities are doing a better job than others. His organization recently published a report on the future of senior living in light of the pandemic.
It calls on operators to institute a host of changes, including establishing safe visiting areas for families both inside and outside; providing high-speed internet services throughout communities; and ensuring adequate supplies of masks and other forms of personal protective equipment for residents and staff, among other recommendations.
Some families now wish they’d arranged for older relatives to receive care in a more structured environment before the pandemic started. They’re finding that older relatives living independently, especially those who are frail or have mild cognitive impairments, are having difficulty managing on their own.
“I’m hearing from a lot of people — mostly older daughters — that we waited too long to move Mom or Dad, we had our head in the sand, can you help us find a place for them,” said Allie Mazza, who owns Brandywine Concierge Senior Services in Kennett Square, Pennsylvania.
While many operators instituted move-in moratoriums early in the pandemic, most now allow new residents as long as they test negative for COVID-19. Quarantines of up to two weeks are also required before people can circulate in the community.
Many older adults, however, simply don’t have the financial means to make a move. More than half of middle-income seniors — nearly 8 million older adults — can’t afford independent living or assisted living communities, according to a study published last year. And more than 7 million seniors are poor, according to the federal Supplemental Poverty Measure, which includes out-of-pocket medical expenses and other drains on cash reserves.
Questions to Ask
For those able to consider senior housing, experts suggest you ask several questions:
How is the facility communicating with residents and families? Has it had a COVID outbreak? Is it disclosing COVID cases and deaths? Is it sharing the latest guidance from federal, state and local public health authorities?
What protocols have been instituted to ensure safety? “I’d want to know: Do they have a plan in place for disasters — not just the pandemic but also floods, fires, hurricanes, blizzards?” Milner said. “And beyond a plan, do they have supplies in place?”
How does the community engage residents? Is online programming — exercise classes, lectures, interest group meetings — available? Are one-on-one interactions with staffers possible? Are staffers arranging online interactions via FaceTime or Zoom with family? Are family visits allowed? “Social engagement and stimulation are more important than ever,” said David Schless, president of the American Seniors Housing Association.
What’s the company’s financial status and occupancy rate? “Properties with occupancy rates of 90% or higher are going to be able to withstand the pressures of COVID-19 significantly more than properties with occupancy below 80%, in my opinion,” said Mace of the National Investment Center for Seniors Housing & Care. Higher occupancy means more revenues, which allows institutions to better afford extra expenses associated with the pandemic.

 ):
):