A smattering of plutonium atoms embedded in Earth’s crust are helping to resolve the origins of nature’s heaviest elements.
Scientists had long suspected that elements such as gold, silver and plutonium are born during supernovas, when stars explode. But typical supernovas can’t explain the quantity of heavy elements in our cosmic neighborhood, a new study suggests. That means other cataclysmic events must have been major contributors, physicist Anton Wallner and colleagues report in the May 14 Science.
The result bolsters a recent change of heart among astrophysicists. Standard supernovas have fallen out of favor. Instead, researchers think that heavy elements are more likely forged in collisions of two dense, dead stars called neutron stars, or in certain rare types of supernovas, such as those that form from fast-spinning stars (SN: 5/8/19).
Heavy elements can be produced via a series of reactions in which atomic nuclei swell larger and larger as they rapidly gobble up neutrons. This series of reactions is known as the r-process, where “r” stands for rapid. But, says Wallner, of Australian National University in Canberra, “we do not know for sure where the site for the r-process is.” It’s like having the invite list for a gathering, but not its location, so you know who’s there without knowing where the party’s at.
Scientists thought they had their answer after a neutron star collision was caught producing heavy elements in 2017 (SN: 10/16/17). But heavy elements show up in very old stars, which formed too early for neutron stars to have had time to collide. “We know that there has to be something else,” says theoretical astrophysicist Almudena Arcones of the Technical University of Darmstadt, Germany, who was not involved with the new study.
If an r-process event had recently happened nearby, some of the elements created could have landed on Earth, leaving fingerprints in Earth’s crust. Starting with a 410-gram sample of Pacific Ocean crust, Wallner and colleagues used a particle accelerator to separate and count atoms. Within one piece of the sample, the scientists searched for a variety of plutonium called plutonium-244, which is produced by the r-process. Since heavy elements are always produced together in particular proportions in the r-process, plutonium-244 can serve as a proxy for other heavy elements. The team found about 180 plutonium-244 atoms, deposited into the crust within the last 9 million years.
Scientists analyzed a sample of Earth’s deep-sea crust (shown) to search for atoms of plutonium and iron with cosmic origins.Norikazu Kinoshita
Researchers compared the plutonium count to atoms that had a known source. Iron-60 is released by supernovas, but it is formed by fusion reactions in the star, not as part of the r-process. In another, smaller piece of the sample, the team detected about 415 atoms of iron-60.
Plutonium-244 is radioactive, decaying with a half-life of 80.6 million years. And iron-60 has an even shorter half-life of 2.6 million years. So the elements could not have been present when the Earth formed, 4.5 billion years ago. That suggests their source is a relatively recent event. When the iron-60 atoms were counted up according to their depth in the crust, and therefore how long ago they’d been deposited, the scientists saw two peaks at about 2.5 million years ago and at about 6.5 million years ago, suggesting two or more supernovas had occurred in the recent past.
The scientists can’t say if the plutonium they detected also came from those supernovas. But if it did, the amount of plutonium produced in those supernovas would be too small to explain the abundance of heavy elements in our cosmic vicinity, the researchers calculated. That suggests regular supernovas can’t be the main source of heavy elements, at least nearby.
That means other sources for the r-process are still needed, says astrophysicist Anna Frebel of MIT, who was not involved with the research. “The supernovae are just not cutting it.”
The measurement gives a snapshot of the r-process in our corner of the universe, says astrophysicist Alexander Ji of Carnegie Observatories in Pasadena, Calif. “It’s actually the first detection of something like this, so that’s really, really neat.”
It’s now open season for COVID-19 vaccines across the United States.
After months of having to scramble to find a shot, the tables have turned and most people who want one can get one. Everyone 16 years and older is eligible for a vaccine, and the U.S. Food and Drug Administration on May 10 extended emergency use authorization for Pfizer’s jab to those aged 12 to 15 years old (SN: 5/10/21).
So far, nearly 60 percent of adults 18 years and older — or around 150 million people — have gotten at least one dose as of May 10. President Joe Biden has set a goal of 70 percent of adults, or around 180 million, getting at least one dose by July 4, and 160 million adults being fully vaccinated — at least two weeks beyond their last shot — by that date.
But with supply beginning to outstrip demand in many parts of the country, that goal could be difficult to reach. Local officials already are launching innovative ways to reach people who are hesitant to get the shot, from going door-to-door to address people’s concerns to promising a free beer or baseball game ticket with each jab.
How many people get the shots will influence when life in the United States might approach something resembling a pre-pandemic normal. Computer simulations showed that if up to 75 percent of eligible people are on track to get vaccinated by September, there could be a sharp drop in cases of COVID-19 even earlier, by July, researchers report May 5 in Morbidity and Mortality Weekly Report. That decline may happen even as health officials loosen some public health guidelines, the simulations showed.
The U.S. Centers for Disease Control and Prevention has already revised mask-wearing recommendations for people who are fully vaccinated. And on May 9, Anthony Fauci, Biden’s top medical adviser for the pandemic, suggested during an interview on ABC’s “This Week” that as vaccinations rise and daily new cases drop, requirements for wearing masks indoors could ease.
“We are not out of the woods yet,” CDC Director Rochelle Walensky said in a news conference on May 5. “But we could be very close.”
As we enter this new phase of the pandemic in the United States — amid a push to get doses to as many willing (or willing-to-be-convinced) people as possible — here are some of the big outstanding questions about vaccines.
How long does immunity last?
The short answer is that researchers don’t know yet. But studies suggest that for most people, antibodies that recognize the coronavirus can last at least a year after an infection —perhaps longer (SN: 11/24/20). And evidence is building that vaccines provide superior protection than natural infection, so it’s not unreasonable to expect that immunity might be longer-lasting for vaccinated people.
One small study, for instance, found that of 19 people tested for antibodies a year after getting sick with COVID-19,17 people still had detectable levels, researchers report in a preliminary study posted May 2 at medRxiv.org. Those who had more severe COVID-19 symptoms were more likely to have higher antibody levels, the researchers found. So it’s possible that people who had mild infections may become susceptible to getting infected again sooner than severely ill individuals.
If I didn’t have side effects after getting the vaccine, is it working?
This is the most common question people ask Juliet Morrison, a virologist at the University of California, Riverside. “Everyone keeps saying, ‘I didn’t feel anything. Am I protected?’”
Morrison reassures her questioners with data. In Moderna’s 30,000-person trial, about 79 percent of people who got the vaccine had whole-body, or systemic, side effects, most commonly headache, fatigue and muscle aches. Some had chills or fever. That left more than 20 percent of people who didn’t have bad side effects beyond an achy arm, or sometimes no side effects at all. But the vaccine’s efficacy was 94 percent. “That’s pretty compelling evidence that you do not need to have the adverse effects to develop immunity against SARS-CoV-2,” Morrison says.
About 37 percent of people in the placebo group in Moderna’s trial also reported systemic side effects. “That might suggest some people have adverse reactions just as a result of the process of receiving an injection, or they might have psyched themselves up about receiving the vaccine,” she says.
Many of the side effects are produced by immune responses that aren’t responsible for building lasting immunity, says Brianne Barker, an immunologist at Drew University in Madison, N.J. “Just because you’re not inducing the particular response that leads to fever, doesn’t mean you aren’t inducing the part that we’re hoping to induce with the vaccine.”
Should I get an antibody test to tell if the vaccine worked?
No. That’s not recommended because many of the antibody tests on the market now don’t test for antibodies like those made after getting vaccinated. Antibody tests usually test for antibodies against the virus’s nucleocapsid, or N protein. Some also test for antibodies against the coronavirus’ spike protein. Such tests are used to determine whether people have had SARS-CoV-2 infections in the past.
Since the vaccines contain only the spike protein, people who have been vaccinated but never had COVID-19 would not have antibodies directed against the N protein. They would get a negative result or indeterminate result from tests that detect N protein antibodies.
“You just need to trust that the efficacy of these vaccines is very high,” Morrison says.
If I have had COVID-19, do I need to be vaccinated?
“All of the evidence says yes,” Barker says. “The immune response you make when you’re infected with SARS-CoV-2 is not ideal.”
That’s because at least four of the coronavirus’s proteins inhibit immune responses and may damage the ability to make lasting immune memories. Studies also indicate that people who have gotten two doses of an mRNA vaccine make more neutralizing antibodies — the kind that help prevent the virus from entering cells — than people who have recovered from COVID-19.
“The immunity the vaccines confer is much more robust than the immunity from an infection,” Morrison says. “The vaccines that we have do a much better job than natural infection does.”
Scientists are still debating whether people who had previous infections need both doses of the mRNA vaccines or if they can get away with just one dose (SN: 3/3/21). For logistical reasons, health officials are currently advising that everyone get the recommended number of doses for the vaccine they’re given (two doses for the mRNA vaccines, one for Johnson & Johnson).
People who got sick and were treated with monoclonal antibodies or with convalescent plasma should wait 90 days before getting a COVID-19 vaccine, as these therapies can otherwise interfere with the immune response, says Matthew Laurens, a pediatric infectious diseases physician and vaccine researcher at the University of Maryland School of Medicine in Baltimore.
Can the vaccine help people recover from long COVID?
Some anecdotal and preliminary evidence suggests it might. About 30 percent to 40 percent of people who have persistent symptoms, known as post-acute sequelae of COVID (PASC), or long- COVID, say they feel better after vaccination.
Exactly why that is isn’t known. One hypothesis is that people with long-COVID never quite cleared the infection. Vaccination may help give any lingering virus the boot. Or it may give the immune system a reset.
Researchers are launching clinical trials to test whether vaccination really can help with the long-term symptoms.
Can the current vaccines protect me from variants?
For the variants that have emerged so far, antibodies sparked by the COVID-19 vaccines used in the United States still seem to do their job and protect people from the worst of the disease. And the shots seem to provide superior protection against variants than previous infections do, Fauci said in a news conference on May 5.
Studies of Pfizer’s vaccine in Israel suggest it ishighly effective against a variant first identified in the United Kingdom, called B.1.1.7 (SN: 4/19/21). In Qatar, Pfizer’s shot was89.5 percent effective against COVID-19 symptoms for infections caused by that variant, researchers report May 5 in the New England Journal of Medicine. For a variant that was first identified in South Africa — called B.1.351 — the vaccine was 75 percent effective against symptomatic COVID-19, the team found. That’s heartening news because the variant hasa mutation that helps the virus evade antibodies to infect lab-grown cells (SN: 1/27/21). The shot’s effectiveness to prevent severe disease or death caused by both variants was even higher, coming in at 97.4 percent.
Some vaccine developers are making moves to update their shots. Moderna, for example, announced May 5 that giving people a third doseboosted the immune response against variants first identified in South Africa and Brazil. Participants in the trial either received a third dose of the original vaccine or an adapted one based on the variant identified in South Africa. Those who got the adapted version had antibodies that were better at stopping the variant viruses from infecting cells compared with the antibodies from people who got a third dose of the original formulation.
Moderna is also testing a version that includes an equal mix of the original strain and the variant from South Africa.
Is it possible to reach herd immunity?
In short, we still don’t know. But achieving herd immunity in the United States is seeming much harder as the pace of vaccinations slows and more contagious variants loom.
Long held up as the ultimate end of the pandemic, herd immunity is the proportion of a population that must be immune to prevent the virus from spreading. When the average infected person spreads the virus to less than one other person, herd immunity is reached and small outbreaks can’t balloon out of control.
Early on, estimates of the threshold needed to reach herd immunity estimates ranged from 60 percent to 70 percent of a population. That number stemmed from initial estimates of the contagiousness of the virus. But viruses can change, and estimates have ticked above 80 percent as more worrisome variants, like B.1.1.7, which is up to 70 percent more transmissible, gain steam (SN: 4/19/21). That variant is now the dominant one causing coronavirus infections in the United States.
It will take exceeding the theoretical threshold to reach herd immunity in the real world. That’s because vaccines aren’t 100 percent effective. And scientists still aren’t sure how well, or durably, they prevent someone from transmitting the virus, although there are tantalizing hints that vaccinated people who do get infected carry less virus and so are less infectious (SN: 2/12/21) . Even with a maximally effective vaccine, there may not be enough people willing to take it to reach herd immunity. According to recent polls, about 25 to 30 percent of Americans express reluctance to get the vaccine.
Biden’s goal of vaccinating 70 percent of adults with at least one shot by July 4 includes about 55 percent of the total population. That likely wouldn’t push us over the herd immunity threshold, but it would still help curb the pandemic. In Israel, for instance, about 60 percent of their population is now vaccinated and cases have dropped significantly and daily deaths have dropped to near zero in recent weeks.
“You vaccinate enough people, the infections are going to go down,” Fauci told the New York Times.
As vaccines to protect people from COVID-19 started becoming available in late 2020, the rhetoric of anti-vaccine groups intensified. Efforts to keep vaccines out of arms reinforce misinformation about the safety and effectiveness of the vaccines and spread disinformation — deliberately misleading people for political, ideological or other reasons.
Vaccines have been met with suspicion and hostility for as long as they have existed. Current opposition to COVID-19 vaccines is just the latest chapter in this long story. The primary driver of vaccine hesitancy throughout history has not been money, selfishness or ignorance.
“Vaccine hesitancy has less to do with misunderstanding the science and more to do with general mistrust of scientific institutions and government,” says Maya Goldenberg, a philosophy expert at the University of Guelph, Ontario, who studies the phenomenon. Historically, people harmed or oppressed by such institutions are the ones most likely to resist vaccines, adds Agnes Arnold-Forster, a medical historian at the University of Bristol in England.
A range of recurring and intersecting themes have fueled hesitancy globally and historically. These include anxiety about unnatural substances in the body, vaccines as government surveillance or weapons, and personal liberty violations. Other concerns relate to parental autonomy, faith-based objections, and worries about infertility, disability or disease. For example, some people oppose vaccines that were grown in cell culture lines that began from aborted fetal cells, or they mistakenly believe vaccines contain fetal cells. One of today’s false beliefs — that COVID-19 vaccines contain a microchip — represents anxiety about both vaccine ingredients and vaccines as a surveillance tool.
“The reasons people have hesitated reflect the cultural anxieties of their time and place,” Goldenberg says. People worried about toxins arising during environmentalism in the 1970s and people in countries steeped in civil war have perceived vaccines as government weapons.
Historical attempts to curb vaccine hesitancy often failed because they relied on authoritarian and coercive methods. “They were very blunt, very punitive and very ineffective,” Arnold-Forster says. “They had very little impact on actual vaccine intake.”
The most effective remedies center on building trust and open communication, with family doctors having the greatest influence on people’s decision to vaccinate. Increased use of “trusted messengers” to share accurate and reassuring vaccine information with their communities builds on this.
18th Century Smallpox vaccine sets the stage around the globe
In a way, anti-vaccination attitudes predate vaccination itself. Public vaccination began after English physician Edward Jenner learned that milkmaids were protected from smallpox after exposure to cowpox, a related virus in cows. In 1796, Jenner scientifically legitimized the procedure of injecting people with cowpox, which he termed variolae vaccinae, to prevent smallpox. However, variolation — which staved off serious smallpox infections by triggering mild infection through exposure to material from an infected person — dates back to at least the 1000s in Asia, Africa and other parts of the world. In some cases people inhaled the dried scabs of smallpox lesions or rubbed or injected pus from smallpox lesions into a healthy person’s scratched skin.
About 1 to 2 percent of people — including a son of Britain’s King George III in 1783 — died from the procedure, far fewer than the up to 30 percent who died from smallpox. Benjamin Franklin rejected variolation, but later regretted it when smallpox killed his youngest son. Onesimus, an enslaved man in Boston, taught the procedure to Puritan minister Cotton Mather, who in turn urged doctors to inoculate the public during a 1721 smallpox outbreak. Many refused, and Mather faced hostility: A small bomb was thrown through his window. Reasons given for avoiding variolation — particularly that it was unnatural to interfere with a person’s relationship with God — were the seeds of later anti-vaccination attitudes.
19th Century The first vaccination laws kindle resistance
In 1809, Massachusetts passed the world’s first known mandatory vaccination law, requiring the general population to receive the smallpox vaccine. Resistance began to grow as other states passed similar laws. Then the U.K. Vaccination Act of 1853 required parents to get infants vaccinated by 3 months old, or face fines or imprisonment. The law sparked violent riots and the formation of the Anti-Vaccination League of London. Vaccine resisters were often poor people suspicious of a forced medical intervention since, under normal circumstances, they rarely received any health care. Anti-vaccination groups argued that compulsory vaccination violated personal liberty, writing that the acts “trample upon the right of parents to protect their children from disease” and “invaded liberty by rendering good health a crime.”
This 1838 illustration seems to take a negative view of a vaccination method that used cowpox to immunize people against a similar, and deadly, human disease, smallpox.National Library of Medicine
Anti-vaccination sentiment grew and spread across Europe until an 1885 demonstration of about 100,000 people in Leicester, England, prompted the British monarchy to appoint a commission to study the issue. The resulting 1896 report led to an 1898 act that removed penalties for parents who didn’t believe vaccination was safe or effective. The act introduced the term “conscientious objectors,” which later became more commonly associated with those who refuse military service on religious or moral grounds.
Across the Atlantic, most U.S. residents had embraced Jenner’s cowpox protective, leading to a precipitous drop in smallpox outbreaks. But with fewer outbreaks, complacency set in and vaccination rates dropped. As smallpox outbreaks resurfaced in the 1870s, states began enforcing existing vaccination laws or passing new ones. British anti-vaccinationist William Tebb visited New York in 1879, which led to the founding of the Anti-Vaccination Society of America. The group’s tactics will sound familiar: pamphlets, court battles and arguments in state legislatures that led to the repeal of mandatory vaccination laws in seven states. The 1905 Supreme Court decision Jacobson v. Massachusetts upheld a state’s right to mandate vaccines; it remains precedent today.
20th Century A menu of vaccines draws praise and ire
1982: Documentary hypes vaccine injuries
The U.S. entered a golden age of vaccine development from the 1920s through the 1970s with the arrival of vaccines for diphtheria, pertussis, polio, measles, mumps and rubella. Opposition diminished as infection rates, particularly for polio, fell. Rosalynn Carter and Betty Bumpers, the wives of the governors of Georgia and Arkansas, respectively, began a vaccination campaign that grew into a national effort in the 1970s. The goal was to encourage every state to require children attending public school to receive most vaccines recommended by the U.S. Centers for Disease Control and Prevention.
A nationally aired 1982 news documentary called “DPT: Vaccine Roulette” changed everything. Lea Thompson, a reporter with WRC-TV in Washington, D.C., shared emotional stories of parents claiming their children had suffered seizures and brain damage from the diphtheria-pertussis-tetanus, or DPT, shot. Interviews with doctors lent the stories credence. Fever-caused seizures were a known side effect of DPT, and a 1974 study had reported neurological complications developing in 36 children within 24 hours of DPT vaccination. But the study did not follow the children long-term. Later research revealed neither the seizures nor the vaccine caused long-term brain damage.
But the damage to public trust was done. Coopting the DPT acronym, one parent, Barbara Loe Fisher, cofounded Dissatisfied Parents Together, which became the National Vaccine Information Center, the most influential anti-vaccine organization in the United States.
1998: Fraudulent study links vaccines to autism
The National Vaccine Information Center maintained a steady hum of anti-vaccination sentiment and activity through the 1980s and ’90s. Then British gastroenterologist Andrew Wakefield published a report in the Lancet alleging that the measles-mumps-rubella, or MMR, vaccine caused autism spectrum disorder in 12 children. Wakefield falsified data, violated informed consent and secretly invested in development of a solo measles vaccine, but it took years to uncover his deceit (SN Online: 2/3/10). Fears about autism and vaccines had already exploded by the time the study was retracted 12 years after publication.
Almost immediately after publication of the study, U.K. vaccination rates began falling. But news of Wakefield’s work didn’t reach the United States until 2000, just as U.S. medical authorities were embroiled in a debate about the use of thimerosal, a mercury-containing preservative, in vaccines. In 1999, the U.S. Public Health Service recommended removing thimerosal from childhood vaccines as a precautionary measure to reduce infants’ mercury exposure. Later research showed no safety concerns about its use.
The MMR vaccine never contained thimerosal, but fears about mercury-related brain damage merged with those about MMR and autism, creating a storm of anger and fear surrounding claims of vaccine harm.
Protesters at a February 2021 event in Sydney, Australia, came out against the idea of mandatory COVID-19 vaccinations, just days before vaccines became available to frontline health care workers.Brook Mitchell/Getty Images
21st Century Social media and slick documentaries
Despite the 2010 retraction of his study and the revocation of his license to practice medicine in the United Kingdom, Wakefield remains a leader in today’s anti-vaccination movement. Joining him is Robert F. Kennedy, Jr., who gained prominence promoting unfounded allegations about thimerosal. Both men rode the wave of anti-vaccination networking on social media and the promotion of disinformation through slick documentaries like 2016’sVaxxed: From Cover-Up to Catastrophe (SN Online: 4/1/16).
In 2014, the United States saw its highest number of measles cases since the disease was eliminated from the country in 2000, culminating in a large outbreak that began at Disneyland that December. In response, California passed a law removing parents’ ability to opt out of vaccinating their children based on personal beliefs and required that all children receive CDC-recommended vaccines to attend school (SN Online: 7/2/19). Extreme opposition to that law and subsequent ones helped fuel a resurgence in anti-vaccine advocacy along with an alarming measles outbreak in 2019 (SN: 12/21/19 & 1/4/20, p. 24).
The vast majority of people accept recommended vaccines and their role in stemming the spread of infectious diseases. Recent surveys suggest that 69 percent of U.S. adults say they have or will get a COVID-19 vaccine, an improvement over the 60 percent willing to do so in November. But responses to surveys don’t necessarily predict behavior, Goldenberg says.
The chemistry leading to life may start before stars are even born.
In the planet-forming disk of gas and dust around a young star, astronomers have detected methanol. The disk is too warm for the methanol to have formed there, so this complex organic molecule probably originated in the interstellar cloud that collapsed to form the star and its disk, researchers report online May 10 in Nature Astronomy. This finding offers evidence that at least some organic matter from interstellar space can seed the disks around newborn stars to provide potential ingredients for life on new planets.
“That’s pretty exciting, because it means that, in principle, all planets forming around any kind of star could have this material,” says Viviana Guzmán, an astrochemist at the Pontifical Catholic University of Chile in Santiago not involved in the work.
Complex organic molecules have been observed in interstellar clouds of gas and dust (SN: 3/22/21), as well as in planet-forming disks around young stars (SN: 2/18/08). But astronomers didn’t know whether organic material from interstellar space could survive the formation of a protoplanetary disk, or whether organic chemistry had to start from scratch around new stars.
“When you form a star and its disk, it’s not a very easy, breezy process,” says Alice Booth, an astronomer at Leiden University in the Netherlands. Radiation from the new star and shock waves in the imploding material, she says, “could destroy a lot of the molecules that were originally in your initial cloud.”
Using the ALMA radio telescope array in Chile, Booth and colleagues observed the disk around a bright, young star named HD 100546, about 360 light-years away. There, the team spotted methanol, which is thought to be a building block for life’s molecules, such as amino acids and proteins.
Methanol could not have originated in the disk, because this molecule forms when hydrogen interacts with carbon monoxide ice, which freezes below temperatures of about –253° Celsius. The disk around HD 100546 is much warmer than that, heated by a star whose surface is roughly 9,700° C — some 4,000 degrees hotter than the sun. So the disk must have inherited its methanol from the interstellar cloud that forged its central star, the researchers conclude.
“This is the first evidence that the really interesting chemistry we see early on [in star formation] actually survives incorporation into the planet-forming disk,” says Karin Öberg, an astrochemist at Harvard University who was not involved in the work. Astronomers should next search the disks around other young stars for methanol or other organic molecules, she says, to “explore whether this is a one-time, get lucky kind of thing, or whether we can safely assume that planet-forming disks always inherit these kinds of molecules.”
PUNE, India — Mohanish Ellitam watched helplessly as his 49-year-old mother’s oxygen levels dipped dangerously and she gasped for air. “I could see her stomach rising and falling,” Ellitam said. “I was so scared.”
Watching his mother’s health deteriorate, Ellitam knew he couldn’t wait any longer. But in Shevgaon, a small town in the state of Maharashtra, health care facilities were limited and already overwhelmed with people suffering from COVID-19. He frantically called friends, family and almost everyone on his contact list with connections to the region’s hospitals. After nearly 100 calls, on April 12 Ellitam finally found a spot at Surabhi Hospital in Ahmednagar, nearly 60 kilometers from his hometown.
But there was no room for relief just yet. His father, 53, also started growing tired and breathless. While his father stayed isolated in a hotel room opposite the hospital, Ellitam lived out of his car parked nearby, and the frustrating search for another hospital bed began.
“I was in a helpless state,” he said. “I felt alone. I broke into tears many times.”
This is what it’s like to be in the hardest-hit state in the country now hit hardest by the coronavirus pandemic. Although Ellitam’s father secured a bed in Surabhi Hospital a day later, scenes like this — and far worse — are playing out hundreds of thousands of times every day across India. As its second wave of COVID-19 sweeps through, India recorded more than 400,000 daily new cases on May 6 — the largest single-day spike in the world — and its highest daily death toll of 4,187, a day later. Those numbers are predicted to soar even higher in the coming days.
Dire SOS pleas from doctors, patients and their loved ones in need of hospital beds, oxygen and medication have flooded social media platforms. In Pune, one of the worst-hit cities in India, the wailing sirens of ambulances have become a macabre feature of the city’s soundscape. In many parts of the country, family members are shedding tears of despair outside of hospitals as they beg for medical attention for their dying kin.
“We don’t have enough ward beds, we don’t have enough ICU beds, and we’re running out of ventilators,” said Sumit Ray, a critical care specialist at Holy Family Hospital in India’s capital city of New Delhi. “People are coming into the ER requiring huge amounts of oxygen support, and we were on the edge of running out.”
Like many others in India, Ray is somewhat baffled by the seemingly sudden COVID-19 surge. In an unprecedented move, hundreds of scientists sent a plea on April 30 to Prime Minister Narendra Modi asking to ramp up data collection and allow access to already collected COVID-19 data. These scientists say more data are needed to understand how the coronavirus is spreading, manage the outbreak and predict what’s to come.
“It is essential now, more than ever before, that dynamic public health plans be implemented on the basis of scientific data to arrest the spread of infections and save the lives of our citizens,” they wrote. As of May 6, more than 800 scientists had signed on to that appeal.
How did we get here?
During the first wave of the pandemic in 2020, India reported over 90,000 daily new COVID-19 cases at its peak, with the highest single-day record at 97,894 on September 16. Daily case numbers then gradually declined to nearly 10,000 in early February.
The falling numbers ignited conversations about whether many Indians, especially those living in densely populated urban centers, might have already been exposed to the virus, thus conferring some immune defenses to prevent reinfection.
In Mumbai — home to more than 20 million people, more than 40 percent of whom live in overcrowded slums where disease can spread like wildfire — blood antibody tests of nearly 7,000 individuals from three municipal wards suggested 57 percent of the sample’s nearly 4,000 slum dwellers had a past infection with COVID-19, researchers reported in the Lancet Global Health in November 2020. In Delhi, similar tests showed that by January 2021, more than half of 28,000 people sampled in 272 municipal wards had developed antibodies against COVID-19 compared with 23 percent of 21,387 people sampled in early 2020.
A national serological survey of over 28,000 participants suggested that 1 in 4 Indians may have been exposed to COVID-19 by December 2020, researchers reported online March 4 on the preprint server SSRN.
“We thought we may not see a big second wave,” said Shahid Jameel, a virologist at Ashoka University in Sonipat, India. “Obviously we were wrong because we didn’t account for both the introductions and indigenous development of new variants.”
In December, India recorded its first six cases of the highly infectious B.1.1.7 variant, which was first identified in the United Kingdom. Between February and March, genetic testing showed that the variant became dominant in India’s northern state of Punjab, appearing in 326 of 401 sequenced viral samples. In New Delhi, B.1.1.7 was present in half the samples sequenced toward the end of March compared with 28 percent two weeks earlier.
India’s own B.1.617 variant first identified in October in Maharashtra is now present in up to 60 percent of samples from some parts of this hard-hit state, according to Jameel. This variant is also spreading in Delhi, he said, in addition to other parts of India and the world.
While B.1.1.7 is thought to be highly transmissible and potentially more lethal than other known variants (SN: 4/19/21), it’s still unclear how contagious B.1.617 is and if it induces severe disease. This makes it challenging to assess its role in India’s increasingly grim situation. One glimmer of hope is that Covaxin, a COVID-19 vaccine administered in India, appears to be effective against the variant, according to a recent paper posted online April 23 at the preprint server bioRxiv.org.
But just how much variants are driving the current surge remains poorly understood because scientists have sequenced viral genetic material from a mere 1 percent of all COVID-19 cases recorded from January to March 2021. “We cannot tell if variants are responsible because we’re not sequencing enough,” said Satyajit Rath, an immunologist associated with the Indian Institute of Science Education and Research in Pune and a signatory on the scientists’ appeal for access to data. “It’s not just inadequate but pathetic.”
A lax attitude toward mask wearing and social distancing in the aftermath of the stringent and prolonged national lockdown from March to June 2020 may also be a big factor in the surge. A misplaced sense of triumph over COVID-19 encouraged gatherings at weddings, political rallies and religious ceremonies. “All those became superspreader events,” Jameel said.
As people mingled and traveled, the virus likely spread and overwhelmed India’s unprepared health care system.
Masking and social distancing took a back seat during celebrations of Holi, the festival of colors, in Hyderabad and across India on March 29, 2021, even as COVID-19 cases surged.Mahesh Kumar A./AP Images
Struggles getting treatments
Many hospitals in the worst-hit parts of India house only severely ill COVID-19 patients. Some states have set up triage centers or “COVID-19 war rooms” to help prioritize patient care and hospitalization amid a grave shortage of resources.
At Mumbai’s P.D. Hinduja Hospital, pulmonologist Lancelot Pinto treats COVID-19 patients but also remotely manages moderately infected individuals, often entire families, who are quarantining at home. He’s seeing fevers that may last longer than a week (compared with just two or three days in the first wave), after which patients either recover or sometimes end up in the hospital due to complicating risk factors such as hypertension and diabetes.
In some cases, doctors are starting stay-at-home patients on steroids like dexamethasone and prednisone right away, in an effort to stave off more serious infections. But that can backfire. Although those drugs have been shown to reduce the risk of death of critically ill patients, they can actually dampen the immune response if given too early in an infection (SN: 9/2/20). That can make it harder for a patient to fight off the virus.
Some patients are also receiving a combination of as many as five to 10 other drugs, which can interact with each other and pose side effects. “We’ve been flabbergasted by the prescriptions we’ve seen throughout the last eight weeks,” Pinto said. “I’ve seen patients who’ve received such a cocktail of drugs deteriorate in their first week of getting admitted.”
Anxious and desperate patients are sometimes requesting — and doctors are sometimes prescribing — unproven treatments. Convalescent plasma therapy is one of them. Early in the pandemic, scientists thought blood plasma from recovered COVID-19 patients could help those newly infected get a jump-start on building up antibodies (SN: 8/25/20). But there’s little evidence the therapy can arrest progression to severe disease. And in India, some doctors are prescribing it as a last-resort measure, often under pressure from patient families who want to ensure they’ve tried everything they could. But several studies have failed to show that convalescent plasma reduces COVID-19 deaths at this late stage of infection.
Some doctors are also prescribing the antimalarial drug hydroxychloroquine. Despite scant evidence for the drug’s effectiveness (SN: 8/2/20), the Indian Council of Medical Research’s latest guidelines for managing COVID-19 still list hydroxychloroquine as a “may use” drug.
Even when a therapy shows some promise, it’s often not easy to get. In April, chaos erupted when the antiviral drug remdesivir, which can potentially shorten the COVID-19 recovery time by a few days but isn’t life-saving, became nearly unavailable (SN: 10/16/20). Some patients and their families resorted to purchasing the drug at two to five times the market price as a black market emerged amid the shortage. The hospital at which Ellitam’s parents were admitted, too, ran out of remdesivir. With help from friends in two different cities, each more than 100 kilometers away, he managed to procure four doses at market price.
In early April, acute shortages of remdesivir in Pune hospitals resulted in long queues outside the Indian city’s pharmacies. Health officials blamed indiscriminate use of the antiviral drug for shortages in Pune and elsewhere.AP Images
Looking forward
An array of mathematicalmodels predict that India’s surge will peak sometime between early and mid-May. Daily case numbers could rise to anywhere between 800,000 and 1 million, and single-day deaths may hit around 5,500 toward the end of the month, said Bhramar Mukherjee, a biostatistician at the University of Michigan in Ann Arbor who has been modeling India’s COVID-19 outbreak since March 2020. “That’s really troubling,” she said.
But these may be overestimates; Mukerjee’s model doesn’t account for the current lockdowns and restrictions that are in place in some states, cities and villages.
To quell case numbers, some public health experts in India say it’s time for a nationwide lockdown, but one that’s more coordinated and humane than the last lockdown. But the unfolding COVID-19 crisis is not just India’s problem; it’s the world’s problem. Rising numbers of infections can provide the virus with greater opportunities to mutate and evolve and thus form new variants (SN: 2/5/21). In a globally connected world, short of draconian lockdowns, it’s hard to contain the spread of infections and new strains. India’s outbreak has already spilled over into neighboring Nepal; other countries, including the United States, are now limiting travelers from India, but it may be too late. B.1.617 has already shown up in the United States and at least 20 other countries.
The crisis could also result in widespread vaccine shortages. India, the world’s largest producer of vaccines, has stopped exports to prioritize domestic needs. Even so, less than 2 percent of Indians are fully vaccinated and less than 9 percent have received their first shot, thanks to a major COVID-19 vaccine shortage. Ramping up vaccination efforts will be key to combating COVID-19, but it’s unlikely to pull India out of the current crisis.
Back in Shevgaon, Ellitam’s parents have recovered and returned home. But he is now battling the virus himself, lying in the same hospital where his parents spent nearly 10 days. Although he has a cough and is fatigued with moderate symptoms, he’s spending several hours every day making phone calls to help others find ventilator- and oxygen-supported hospital beds for their loved ones.
“The situation here is very bad,” he said. “I pray that no one ever goes through times like these.”
Placebos can make us feel better. Mild electric zaps to the brain can make that effect even stronger, scientists report online May 3 in Proceedings of the National Academy of Sciences. The finding raises the possibility of enhancing the power of expectations to improve treatments.
This is the first study to boost placebo and blunt pain-inducing nocebo effects by altering brain activity, says Jian Kong, a pain researcher at Massachusetts General Hospital in Charlestown.
The placebo effect arises when someone feels better after taking an inactive substance, like a sugar pill, because they expect the substance to help. The nocebo effect is the placebo’s evil twin: A person feels worse after taking an inactive substance that they expect to have unpleasant effects.
To play with people’s expectations, Kong’s team primed 81 participants for painful heat. The heat was delivered by a thermal stimulator to the forearm while participants lay in a functional MRI scanner. Each person received three creams, each to a different spot on their arms. One cream, participants were told, was a numbing lidocaine cream, one was a regular cream and one was a pain-increasing capsaicin cream. But in fact, all the creams were the same inert lotion, dyed different colors.
Participants reported lower pain intensity from the heat on the “lidocaine” patch of skin, an expected placebo effect. People also reported higher pain intensity on the “capsaicin” skin, an expected nocebo effect.
Before testing the placebo and nocebo effects, researchers had delivered electric currents to some participants’ brains with a method called transcranial direct current stimulation, or tDCS. During these tDCS sessions, two electrodes attached to the scalp delivered weak electric current to the brain to change the behavior of brain cells.
Some participants received tDCS targeted at a brain area thought to be important in placebo and nocebo effects, the right dorsolateral prefrontal cortex. Researchers used two types of current: positive anodal tDCS, which typically makes nerve cells more likely to fire off signals, and negative cathodal tDCS, which usually makes cells quieter.
Compared with people who didn’t receive tDCS, people who received cathodal tDCS reported stronger placebo effects when heat was applied to the skin with “lidocaine” cream. For people who received anodal tDCS, the stimulation dampened the nocebo effect of the “capsaicin” cream.
Brain stimulation affected neural pathways that were already thought to be involved in the placebo and nocebo effects. Cathodal tDCS, for instance, boosted connections between the targeted brain area with a nearby area involved in emotion and cognition. This strengthened pattern correlated with participants reporting a stronger placebo effect, Kong and his colleagues found.
“This is a very elegant study and I’m very excited and enthusiastic about it,” says Luana Colloca, a neuroscientist at the University of Maryland Baltimore. Colloca, who wasn’t involved in the study, sees the potential to help chronic pain patients by ramping up the placebo effect (SN: 9/13/18). “We’re not there yet,” she cautions. “We need to see if these same results can be replicated in patients with chronic pain.”
Kong agrees. His study was small, and people experience pain and placebos differently. “But I have to say, this is also encouraging,” he says.
Earth’s hot springs and hydrothermal vents are home to a previously unidentified group of archaea. And, unlike similar tiny, single-celled organisms that live deep in sediments and munch on decaying plant matter, these archaea don’t produce the climate-warming gas methane, researchers report April 23 in Nature Communications.
“Microorganisms are the most diverse and abundant form of life on Earth, and we just know 1 percent of them,” says Valerie De Anda, an environmental microbiologist at the University of Texas at Austin. “Our information is biased toward the organisms that affect humans. But there are a lot of organisms that drive the main chemical cycles on Earth that we just don’t know.”
Archaea are a particularly mysterious group (SN: 2/14/20). It wasn’t until the late 1970s that they were recognized as a third domain of life, distinct from bacteria and eukaryotes (which include everything else, from fungi to animals to plants).
For many years, archaea were thought to exist only in the most extreme environments on Earth, such as hot springs. But archaea are actually everywhere, and these microbes can play a big role in how carbon and nitrogen cycle between Earth’s land, oceans and atmosphere. One group of archaea, Thaumarchaeota, are the most abundant microbes in the ocean, De Anda says (SN: 11/28/17). And methane-producing archaea in cows’ stomachs cause the animals to burp large amounts of the gas into the atmosphere (SN: 11/18/15).
Now, De Anda and her colleagues have identified an entirely new phylum — a large branch of related organisms on the tree of life — of archaea. The first evidence of these new organisms were within sediments from seven hot springs in China as well as from the deep-sea hydrothermal vents in the Guaymas Basin in the Gulf of California. Within these sediments, the team found bits of DNA that it meticulously assembled into the genetic blueprints, or genomes, of 15 different archaea.
The researchers then compared the genetic information of the genomes with that of thousands of previously identified genomes of microbes described in publicly available databases. But “these sequences were completely different from anything that we know,” De Anda says.
She and her colleagues gave the new group the name Brockarchaeota, for Thomas Brock, a microbiologist who was the first to grow archaea in the laboratory and who died in April. Brock’s discovery paved the way for polymerase chain reaction, or PCR, a Nobel Prize–winning technique used to copy small bits of DNA, and currently used in tests for COVID-19 (SN: 3/6/20).
Brockarchaeota, it turns out, actually live all over the world — but until now, they were overlooked, undescribed and unnamed. Once De Anda and her team had pieced together the new genomes and then hunted for them in public databases, they discovered that bits of these previously unknown organisms had been found in hot springs, geothermal and hydrothermal vent sediments from South Africa to Indonesia to Rwanda.
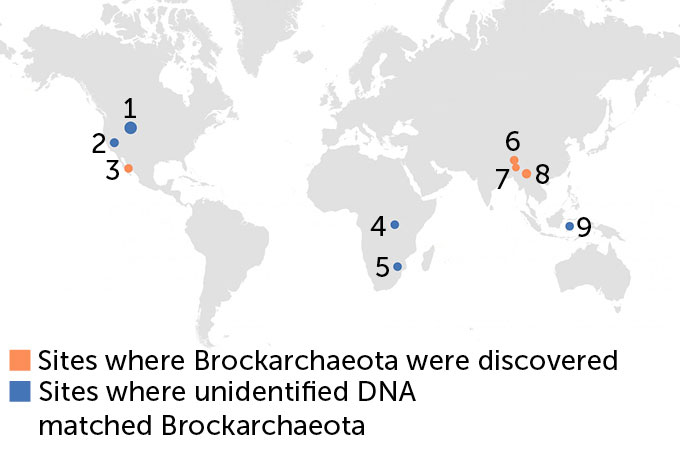
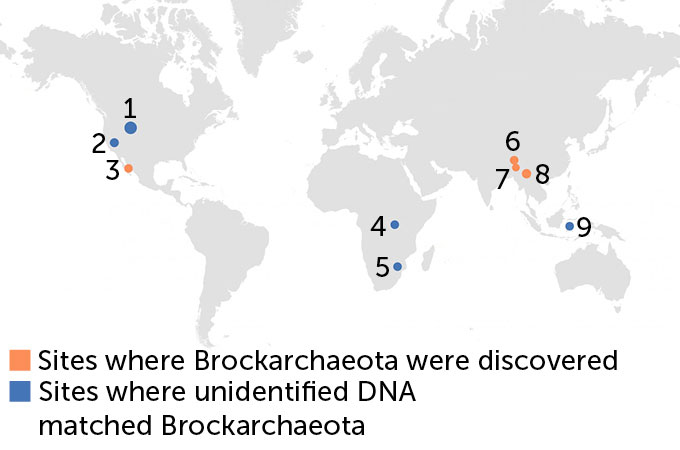
DNA detective work
Sediments collected at hot springs in China and at the Guaymas Basin in the Gulf of California (in orange) contained bits of DNA that scientists found came from a previously undescribed group of organisms, dubbed Brockarchaeota, that also have a unique metabolism. After reconstructing the genetic blueprints of 15 different organisms from this group, the researchers found that fragments of DNA from all over the world (places marked in blue) that researchers had already uploaded to publicly available databases also turned out to belong to this group.
Sites where Brockarchaeota have been found
University of Texas at Austin
1. Yellowstone National Park hot springs (United States) 2. Little Hot Creek hot springs (United States) 3. Guaymas Basin deep sea sediments (Gulf of California) 4. Lake Kivu sediments (Rwanda) 5. South Africa hot springs 6. Qucai and Quzhoumu hot springs (China) 7. Gudui geothermal area hot springs (China) 8. Tengchong hot springs (China) 9. Gulf of Boni lake sediments (Indonesia)
Within the new genomes, the team also hunted for genes related to the microbes’ metabolism — what nutrients they consume and what kind of waste they produce. Initially, the team expected that — like other archaea previously found in such environments — these archaea would be methane producers. They do munch on the same materials that methane-producing archaea do: one-carbon compounds like methanol or methylsulfide. “But we couldn’t identify the genes that produce methane,” De Anda says. “They are not present in Brockarchaeota.”
That means that these archaea must have a previously undescribed metabolism, through which they can recycle carbon — for example in sediments on the seafloor — without producing methane. And, given how widespread they are, De Anda says, these organisms could be playing a previously hidden but significant role in Earth’s carbon cycle.
“It’s twofold interesting — it’s a new phylum and a new metabolism,” says Luke McKay, a microbial ecologist of extreme environments at Montana State University in Bozeman. The fact that this entire group could have remained under the radar for so long, he adds, “is an indication of where we are in the state of microbiology.”
But, McKay adds, the discovery is also a testimonial to the power of metagenomics, the technique by which researchers can painstakingly tease apart individual genomes out of a large hodgepodge of microbes in a given sample of water or sediments. Thanks to this technique, researchers are identifying more and more parts of the previously mysterious microbial world.
“There’s so much out there,” De Anda says. And “every time you sequence more DNA, you start to realize that there’s more out there that you weren’t able to see the first time.”
From lies about election fraud to QAnon conspiracy theories and anti-vaccine falsehoods, misinformation is racing through our democracy. And it is dangerous.
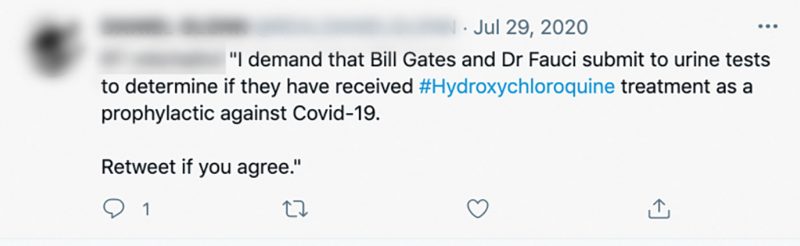
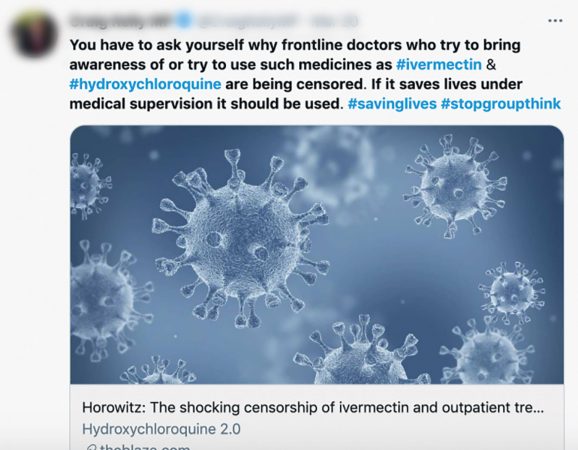
Awash in bad information, people have swallowed hydroxychloroquine hoping the drug will protect them against COVID-19 — even with no evidence that it helps (SN Online: 8/2/20). Others refuse to wear masks, contrary to the best public health advice available. In January, protestors disrupted a mass vaccination site in Los Angeles, blocking life-saving shots for hundreds of people. “COVID has opened everyone’s eyes to the dangers of health misinformation,” says cognitive scientist Briony Swire-Thompson of Northeastern University in Boston.
The pandemic has made clear that bad information can kill. And scientists are struggling to stem the tide of misinformation that threatens to drown society. The sheer volume of fake news, flooding across social media with little fact-checking to dam it, is taking an enormous toll on trust in basic institutions. In a December poll of 1,115 U.S. adults, by NPR and the research firm Ipsos, 83 percent said they were concerned about the spread of false information. Yet fewer than half were able to identify as false a QAnon conspiracy theory about pedophilic Satan worshippers trying to control politics and the media.
Scientists have been learning more about why and how people fall for bad information — and what we can do about it. Certain characteristics of social media posts help misinformation spread, new findings show. Other research suggests bad claims can be counteracted by giving accurate information to consumers at just the right time, or by subtly but effectively nudging people to pay attention to the accuracy of what they’re looking at. Such techniques involve small behavior changes that could add up to a significant bulwark against the onslaught of fake news.
In January, protests closed down a mass vaccination site at Dodger Stadium in Los Angeles.Irfan Khan/Los Angeles Times via Getty Images
Wow factor
Misinformation is tough to fight, in part because it spreads for all sorts of reasons. Sometimes it’s bad actors churning out fake-news content in a quest for internet clicks and advertising revenue, as with “troll farms” in Macedonia that generated hoax political stories during the 2016 U.S. presidential election. Other times, the recipients of misinformation are driving its spread.
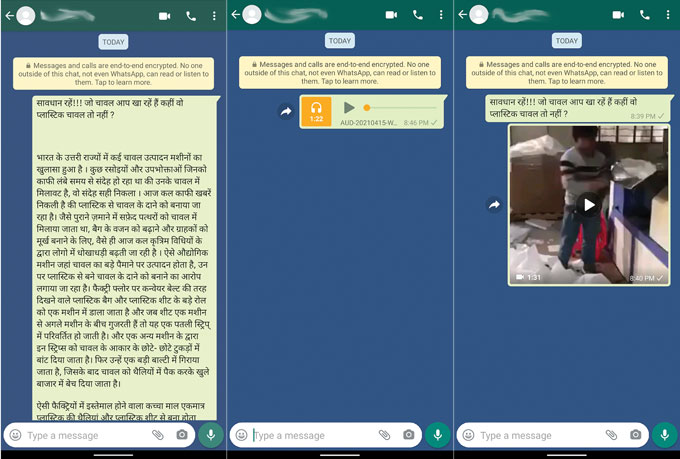
Some people unwittingly share misinformation on social media and elsewhere simply because they find it surprising or interesting. Another factor is the method through which the misinformation is presented — whether through text, audio or video. Of these, video can be seen as the most credible, according to research by S. Shyam Sundar, an expert on the psychology of messaging at Penn State. He and colleagues decided to study this after a series of murders in India started in 2017 as people circulated via WhatsApp a video purported to be of child abduction. (It was, in reality, a distorted clip of a public awareness campaign video from Pakistan.)
Sundar recently showed 180 participants in India audio, text and video versions of three fake-news stories as WhatsApp messages, with research funding from WhatsApp. The video stories were assessed as the most credible and most likely to be shared by respondents with lower levels of knowledge on the topic of the story. “Seeing is believing,” Sundar says.
Video sells
WhatsApp users looked at three versions of a story that falsely claimed that rice was being made out of plastic — in (left to right) text, audio or a video showing a man feeding plastic sheets into a machine.
S.S. Sundar, M.D. Molina and E. Cho
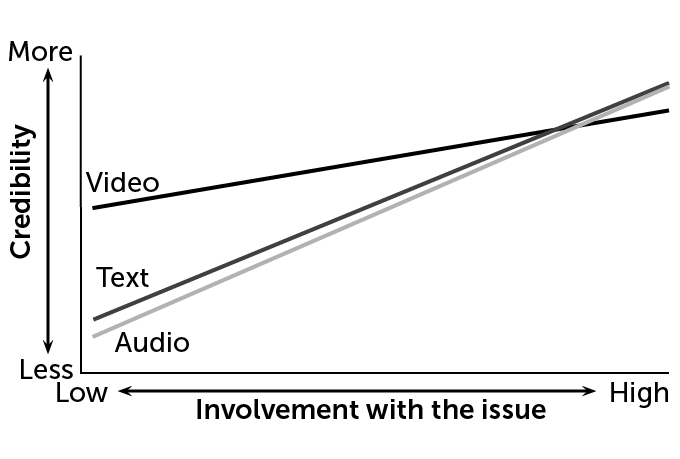
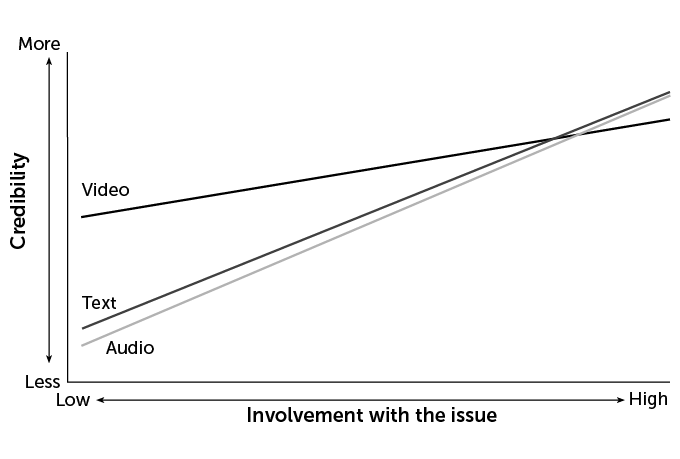
Participants tended to rate the video version as more credible than the audio or text versions. The effect diminished for users who were highly involved with the topic of the false story, suggesting that video is a particularly compelling medium for those who may not be knowledgeable on the topic at hand.
Perceived credibility of a message based on format and issue involvement
T. Tibbitts
T. Tibbitts
Source: S.S. Sundar and E. Cho/Penn State and M. Molina/Michigan State Univ.
The findings, in press at the Journal of Computer-Mediated Communication, suggest several ways to fight fake news, he says. For instance, social media companies could prioritize responding to user complaints when the misinformation being spread includes video, above those that are text-only. And media-literacy efforts might focus on educating people that videos can be highly deceptive. “People should know they are more gullible to misinformation when they see something in video form,” Sundar says. That’s especially important with the rise of deepfake technologies that feature false but visually convincing videos (SN: 9/15/18, p. 12).
One of the most insidious problems with fake news is how easily it lodges itself in our brains and how hard it is to dislodge once it’s there. We’re constantly deluged with information, and our minds use cognitive shortcuts to figure out what to retain and what to let go, says Sara Yeo, a science-communication expert at the University of Utah in Salt Lake City. “Sometimes that information is aligned with the values that we hold, which makes us more likely to accept it,” she says. That means people continually accept information that aligns with what they already believe, further insulating them in self-reinforcing bubbles.
Compounding the problem is that people can process the facts of a message properly while misunderstanding its gist because of the influence of their emotions and values, psychologist Valerie Reyna of Cornell University wrote in 2020 in Proceedings of the National Academy of Sciences.
Thanks to new insights like these, psychologists and cognitive scientists are developing tools people can use to battle misinformation before it arrives — or that prompts them to think more deeply about the information they are consuming.
One such approach is to “prebunk” beforehand rather than debunk after the fact. In 2017, Sander van der Linden, a social psychologist at the University of Cambridge, and colleagues found that presenting information about a petition that denied the reality of climate science following true information about climate change canceled any benefit of receiving the true information. Simply mentioning the misinformation undermined people’s understanding of what was true.
That got van der Linden thinking: Would giving people other relevant information before giving them the misinformation be helpful? In the climate change example, this meant telling people ahead of time that “Charles Darwin” and “members of the Spice Girls” were among the false signatories to the petition. This advance knowledge helped people resist the bad information they were then exposed to and retain the message of the scientific consensus on climate change.
Here’s a very 2021 metaphor: Think of misinformation as a virus, and prebunking as a weakened dose of that virus. Prebunking becomes a vaccine that allows people to build up antibodies to bad information. To broaden this beyond climate change, and to give people tools to recognize and battle misinformation more broadly, van der Linden and colleagues came up with a game, Bad News, to test the effectiveness of prebunking (see Page 36). The results were so promising that the team developed a COVID-19 version of the game, called GO VIRAL! Early results suggest that playing it helps people better recognize pandemic-related misinformation.
Take a breath
Sometimes it doesn’t take very much of an intervention to make a difference. Sometimes it’s just a matter of getting people to stop and think for a moment about what they’re doing, says Gordon Pennycook, a social psychologist at the University of Regina in Canada.
In one 2019 study, Pennycook and David Rand, a cognitive scientist now at MIT, tested real news headlines and partisan fake headlines, such as “Pennsylvania federal court grants legal authority to REMOVE TRUMP after Russian meddling,” with nearly 3,500 participants. The researchers also tested participants’ analytical reasoning skills. People who scored higher on the analytical tests were less likely to identify fake news headlines as accurate, no matter their political affiliation. In other words, lazy thinking rather than political bias may drive people’s susceptibility to fake news, Pennycook and Rand reported in Cognition.
Inattention plays a major role in the spread of misinformation, Pennycook argues. Fortunately, that suggests some simple ways to intervene, to “nudge” the concept of accuracy into people’s minds, helping them resist misinformation. “It’s basically critical thinking training, but in a very light form,” he says. “We have to stop shutting off our brains so much.”
Push in the right direction
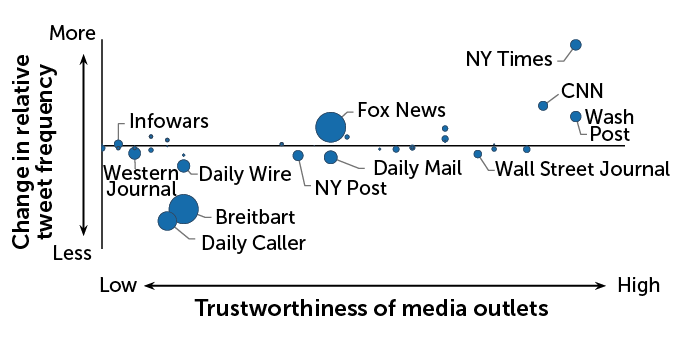
Nudging Twitter users to think about the accuracy of a nonpolitical headline resulted in users temporarily sharing more information from more trustworthy media outlets (blue dots toward the right) and less from less trustworthy outlets (blue dots toward the left). Dot size is proportional to the number of tweets that link to that website prior to the accuracy nudge.
Effect of an accuracy nudge on news sharing
T. Tibbitts
Source: G. Pennycook et al/Nature 2021
With nearly 5,400 people who previously tweeted links to articles from two sites known for posting misinformation — Breitbart and InfoWars — Pennycook, Rand and colleagues used innocuous-sounding Twitter accounts to send direct messages with a seemingly random question about the accuracy of a nonpolitical news headline. Then the scientists tracked how often the people shared links from sites of high-quality information versus those known for low-quality information, as rated by professional fact-checkers, for the next 24 hours.
For debunking, timing can be everything. Tagging headlines as “true” or “false” after presenting them helped people remember whether the information was accurate a week later, compared with tagging before or at the moment the information was presented, Nadia Brashier, a cognitive psychologist at Harvard University, reported with Pennycook, Rand and political scientist Adam Berinsky of MIT in February in Proceedings of the National Academy of Sciences.
How to debunk
Debunking bad information is challenging, especially if you’re fighting with a cranky family member on Facebook. Here are some tips from misinformation researchers:
Arm yourself with media-literacy skills, at sites such as the News Literacy Project (newslit.org), to better understand how to spot hoax videos and stories.
Don’t stigmatize people for holding inaccurate beliefs. Show empathy and respect, or you’re more likely to alienate your audience than successfully share accurate information.
Translate complicated but true ideas into simple messages that are easy to grasp. Videos, graphics and other visual aids can help.
When possible, once you provide a factual alternative to the misinformation, explain the underlying fallacies (such as cherry-picking information, a common tactic of climate change deniers).
Mobilize when you see misinformation being shared on social media as soon as possible. If you see something, say something.
Source: The Debunking Handbook 2020; News Literacy Project
Prebunking still has value, they note. But providing a quick and simple fact-check after someone reads a headline can be helpful, particularly on social media platforms where people often mindlessly scroll through posts.
Social media companies have taken some steps to fight misinformation spread on their platforms, with mixed results. Twitter’s crowdsourced fact-checking program, Birdwatch, launched as a beta test in January, has already run into trouble with the poor quality of user-flagging. And Facebook has struggled to effectively combat misinformation about COVID-19 vaccines on its platform.
Misinformation researchers have recently called for social media companies to share more of their data so that scientists can better track the spread of online misinformation. Such research can be done without violating users’ privacy, for instance by aggregating information or asking users to actively consent to research studies.
Much of the work to date on misinformation’s spread has used public data from Twitter because it is easily searchable, but platforms such as Facebook have many more users and much more data. Some social media companies do collaborate with outside researchers to study the dynamics of fake news, but much more remains to be done to inoculate the public against false information.
“Ultimately,” van der Linden says, “we’re trying to answer the question: What percentage of the population needs to be vaccinated in order to have herd immunity against misinformation?”
The city of Serrana in Brazil is a living experiment.
The picturesque place, surrounded by sugarcane fields, is nestled in the southeast of one of the countries hit hardest by COVID-19. By the end of March, daily deaths in Brazil surged to 3,000 on average a day, a high in a pandemic that has claimed more than 405,000 lives there — the second worst death toll of any country in the world behind only the United States. And as vaccines slowly trickle into the country, only about 15 percent of the population has gotten at least one shot.
Except in Serrana. There, nearly all the adults have gotten their shots. What happens next in this city could provide a glimpse of what the future of the pandemic could be — not only in Brazil but across the globe as vaccinations pick up.
The mass vaccination is an experiment dubbed Projeto S, which will measure the real-world effectiveness of the Chinese-made CoronaVac vaccine, including how well it protects against coronavirus variants. One variant called P.1, which first emerged in the Brazilian Amazon and is now widespread throughout Brazil, shows signs of being both more contagious and able to evade antibodies trained to recognize the coronavirus (SN: 4/14/21).
Among the questions the study may help answer is “whether vaccinated people protect the unvaccinated, how long does their immunity last, and what variants are circulating,” says Marcos Borges, project coordinator and director of the Serrana State Hospital. “We’ll finally be able to observe how a large set of people respond to the vaccine in real-world conditions.”
Projeto S may be the best way to understand the effectiveness of vaccination against COVID-19 in the short and medium terms, says Ethel Maciel, an epidemiologist at the Federal University of Espírito Santo. “This is especially important because we don’t know when we will have most Brazilians vaccinated,” says Maciel, who is not involved in the initiative.
This aerial image shows Serrana, a town of 45,600 people at the north of São Paulo state, where researchers are conducting Projeto S.Andre Penner/AP Images
Setting up the project
Serrana has the perfect ingredients for the Projeto S experiment. It’s relatively small, with 45,600 residents, with roughly 30,000 adults. It’s located near an important public health research center, University of São Paulo’s campus in nearby Ribeirão Preto. And the virus was clearly circulating in the community. A July 2020 study “showed that 5 percent of the population carried the active virus — that is one person in 20, a very high rate,” Borges says.
The town’s residents were eager to be vaccinated, however. When the project launched in February, the team at Instituto Butantan, a research facility and vaccine maker based in São Paulo state that is sponsoring the project, set a goal of vaccinating at least 80 percent of town residents over 18 years old. “We took into account that Brazil has a long tradition of good adhesion to vaccination, so we knew these 80 percent were within reach,” says Borges.
By April 11, 27,722 adult volunteers had gotten the first shot and almost all of them, 27,160, had gotten the second jab by the end of that month, meaning 95.7 percent of Serrana’s adults were fully vaccinated. This success came even as Brazilian president Jair Bolsonaro publicly shunned vaccines — CoronaVac in particular — on several occasions.
The vaccine was developed by China-based Sinovac Biotech. It uses an inactivated, or “killed” version of SARS-CoV-2, the virus that causes COVID-19, that can’t cause illness, but can train the body’s immune system to recognize the coronavirus so it can fight back against an encounter with the real pathogen.
In a Phase III clinical trial with 12,600 health care workers in São Paulo, CoronaVac had an efficacy of roughly 50 percent two weeks after the second dose, researchers report in a preliminary study posted April 15 at medRxiv.org. Fifty percent efficacy is the threshold the U.S. Food and Drug Administration set as a baseline for considering emergency use authorization of COVID-19 vaccines in the United States. In comparison, in clinical trials, the Moderna and Pfizer mRNA vaccines had an efficacy of around 95 percent (SN: 11/16/20; SN: 11/18/20).
Volunteers go through a screening process before enrolling in Projeto S.Divulgação/Instituto Butantan
Like Pfizer’s and Moderna’s vaccines, CoronaVac offers good protection against death and serious forms of COVID-19; of nine health care workers hospitalized with COVID-19, six were unvaccinated, one had had a single dose of CoronaVac and two had gotten both doses. One person —an unvaccinated health care worker — died.
Real-world data
A clinical trial is one thing. The real world is another. For instance, having immunized neighbors might make an important difference in how effective a vaccine actually is. “What is the difference between a vaccine that has 95 percent of individual efficacy and one that has over 50 percent? You’ve got to vaccinate 80 or 85 percent of people with the former to have the disease under control and must vaccinate everyone with the latter to have the same result,” says Ernesto Marques, a virologist at the University of Pittsburgh.
As most adults have been vaccinated in Serrana, Marques says he believes the results will show collective protection — or effectiveness — with CoronaVac, even if individual protection seems low comparatively. This is important not only to Brazil, “but to all countries adopting the vaccine, like Indonesia and Turkey. The results in Serrana will weigh immensely in COVID-19 vaccination policies wherever CoronaVac is used,” he says. Communities in other countries are attempting something similar with other vaccines.
Outcomes may show whether the impact of Serrana’s mass vaccination spills beyond city limits. “Around 15,000 of Serrana’s 45,000 inhabitants commute large distances to work, so we’ll see how it all unfolds with a highly mobile population,” Borges says.
Projeto S is yielding some tantalizing early results. Local media reported that the number of daily COVID-related infections decreased from 28 on March 20 to seven a month later. The share of cases that were severe dropped from a peak of 70 percent this March to 10 percent in early April.
A volunteer gets the second shot of CoronaVac at the Municipal School Jardim Dom Pedro I in Serrana.Divulgação/Instituto Butantan
During the project’s vaccination from mid-February to mid-April, six immunized people died from COVID-19, according to the state government of São Paulo. Of those, five had received only one dose and the other person showed symptoms shortly after receiving the second dose, which leads researchers to believe the patient was already infected at the time of the second shot. Among the unvaccinated there were 14 deaths.
In the beginning of May, none of the six infirmary beds at Serrana’s Santa Casa Hospital and the city’s Basic Healthcare Unit are occupied, and the waiting line for beds both in infirmaries and intensive care units has zeroed. As of May 3, there is one Serrana resident in an infirmary and nine patients in an ICU, according to the Serrana Health Secretariat.
Nurse Glenda de Moraes, who has worked for two decades in Serrana and is involved in the coordination of Projeto S, says that positive test results have dropped, too, “to less than 20 percent [per day], way less than the 30 to 40 percent of positives we had before.”
Still according to the local Health Secretariat, confirmed cases peaked in January 2021, with 706 city residents infected with COVID-19. Infections then decreased in February and March (484 and 692 cases, respectively) and had a sharp drop in April, with 235 confirmed cases.
All of this is clearly “an effect from the vaccination,” Maciel says. But Borges is more cautious in relating all these changes to the mass immunization. “We are still studying it and when we have the results, we’ll be able to affirm for sure if these events are related,” he says.
Projeto S will continue following residents for a year. The questions that tracking can answer — for instance, how long does a vaccine provide protection — are crucial to helping Brazilians, and the rest of the world, find the path out of the pandemic.
Juliana Elaga, the first person to be vaccinated in Serrana, is sure this is the way out. “I suffered a lot with the pandemic, and the vaccination was a really emotional moment for me. I felt truly relieved after the second jab. Even still adopting social distancing and mask-wearing, my heart is more at rest.” Her 8-year-old, Petras, is a witness: “Mom used to wear two masks at once and rub her hands with alcohol-gel all the time. Now she seems a little more normal and not so worried all the time.”
Bad information isn’t new. Propagandists and scam artists have been selling their brand of proverbial snake oil for ages, all to bend people’s thinking to their goals. What’s different today is that the digital world flings information faster and farther than ever before.
Our brains can’t always keep up.
That’s because we often rely on quick estimates to figure out whether something is true. These shortcuts, called heuristics, are often based on very simple patterns (SN: 9/20/14, p. 24). For instance, most information we come across in our daily lives is true. So when forced to guess, we often err on the side of believing.
Other shortcuts exist that encourage information — true or false — to find its way into our minds, research on human psychology shows. We take notice of information that is new, that fires up our emotions, that supports what we already believe and that we hear over and over.
Most of the time, these shortcuts make us “super-efficient,” quickly leading us to the right answer, says cognitive psychologist Elizabeth Marsh of Duke University. But in fast-moving digital landscapes, those shortcuts are “going to get us in trouble,” she says.
How the various online platforms feed us information changes the game, as well. “We are not only contending with our own cognitive crutches as humans,” says Jevin West, a computational social scientist at the University of Washington in Seattle who cowrote the 2020 book Calling Bullshit: The Art of Skepticism in a Data-Driven World. “We’re also contending with a platform, and with algorithms and bots that know how to pierce into our cognitive frailties.” The goal, he says, is “to glue our eyeballs to those platforms.”
Here, scientists who study misinformation pull back the curtain on some false social media posts to show how bad information can creep into our minds.
Sharing what’s new
People take special notice of fresh information. “Novelty has an advantage in the information economy in terms of spreading farther, faster, deeper,” says information scientist Sinan Aral of MIT and author of the 2020 book The Hype Machine: How Social Media Disrupts Our Elections, Our Economy, and Our Health — And How We Must Adapt. Fresh intel can inform our beliefs, behaviors and predictions in powerful ways. In a study of Twitter behavior that spanned 10 years, Aral and his colleagues found more signs of surprise — an indicator that information was new — in people’s responses to false news stories than to true ones.
Sharing new tidbits can also provide a status boost, as any internet influencer knows. “We gain in status when we share novel information,” Aral says. “It makes us look like we’re in the know.”
New information becomes even more alluring in times of uncertainty, West says. That played out early in the COVID-19 pandemic, when researchers and physicians were scrambling to find life-saving treatments. Unproven methods — vitamins, garlic and hydroxychloroquine, among others — got lots of attention. “There were not a lot of answers on how to treat COVID early in the pandemic,” he says.
Misinformation: Natural “cure”
Expert’s review
This tweet provides unequivocal, confident certainty with “cure” and it appeals to people’s beliefs [in natural remedies] with “pawpaw tree” and “garlic.” The author understands well these tricks. The consumer will want to believe this, and … be in the know by seeing it before their friends receive it as a share. — Jevin West, University of Washington
Editor’s note: This box and those below show false statements found on social media or in the news. These examples, all misleading and untrue, show how misinformation can trick us.
Supports prior beliefs
Accepting information that’s consistent with what we already know to be true can feel like a safe bet. We tend to give that sort of message less scrutiny. “It’s more comfortable to find pieces of information that fit our narrative,” West says. “And when we are confronted with information that breaks that narrative, that’s incredibly uncomfortable.”
But this reliance on our stored knowledge can lead us astray. People are wrong about a lot of facts, easily confuse facts and opinions and claim to know facts that are impossible, as Marsh and her colleague Nadia Brashier of Harvard University wrote in 2020 in Annual Review of Psychology. And with so much information streaming in, it’s easy to find the material that fits with what you think you know. “To the extent that I want to believe X, I can go out there and find evidence for X,” Marsh says. “If I were an anti-vaxxer, it wouldn’t matter how many times you told me that vaccines are good, because it would be against my world identity,” she says.
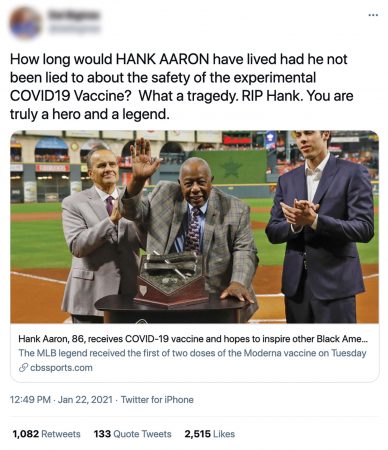
Baseball legend and civil rights advocate Hank Aaron died on January 22 at age 86. Some people soon noted that he’d received a COVID-19 vaccine 17 days earlier. Anti-vaccine groups used his death to blame vaccines, with no evidence that the vaccine was involved. “It’s so opportunistic,” says global health researcher Tim Mackey of the University of California, San Diego.
Misinformation: Sports legend
Expert’s review
This one is very emotive. Most everyone knows Hank Aaron. [The post is] playing on [a] reaction of shock over his death (novel info) and then introducing misinformation that leads people to believe he died from the COVID-19 vaccine. The use of the [CBS Sports] link is compelling as it’s from a trusted news source, even though the link says nothing about Aaron dying from the vaccine. It almost makes him an unknowing martyr for the anti-vax movement. Aaron said he wanted to encourage vaccine uptake among African American people. His untimely death is instead used strategically to target this population. — Tim Mackey, UC San Diego
Tugs on emotions
Playing on emotions is the “dirtiest, easiest trick,” West says.
Outrage, fear and disgust can capture a reader’s attention. That’s what turned up in Aral’s analyses of over 126,000 instances of rumors spreading through tweets, reported in 2018 in Science. False rumors were more likely to inspire disgust than true information, the researchers found.
“False news is shocking, surprising, blood-boiling, anger-inducing,” Aral says. “That shock and awe combines with novelty to really get false news spreading at a much faster rate than true news.” The presence of emotional language increases the spread of social media messages by about 20 percent for each emotion-triggering word, researchers at New York University reported in Proceedings of the National Academy of Sciences in 2017.
Along with message content, readers’ emotions matter, too. People who rely on emotions to assess a news story are more likely to be duped by fake news, misinformation scientist Cameron Martel of MIT and colleagues reported in 2020 in Cognitive Research: Principles and Implications.
Misinformation: Emotions
Expert’s review
[In studies], this headline was particularly evocative of both anger and anxiety, even relative to other false news headlines. I would guess that this has to do with the fact that the headline is tapping into both a common myth about (false) vaccine dangers, and focuses on potential harm to a vulnerable population (children). — Cameron Martel, MIT
On repeat
Even the most outlandish idea begins to sound less wild the 10th time we hear it. That’s been the case since long before the internet existed. In a 1945 study, people were more inclined to believe rumors about wartime rationing that they had heard before rather than unfamiliar ones.
Many recent studies have found similar effects for repetition, a phenomenon sometimes called the “illusory truth effect.” Even when people know a statement is false, hearing it again and again gives it more weight, Marsh says. “Keep it simple. Say it over and over.”
There’s lots of repetition to be found on Twitter, where hashtags can draw many people into a conversation, Mackey says. On July 27, 2020, then-President Donald Trump tweeted a link to a video of a doctor making false claims that hydroxychloroquine can cure COVID-19. Similar tweets exploded soon after, jumping from an average of about 29,000 daily tweets to over a million just a day later, Mackey and his colleagues reported in the Lancet Digital Health in February. “It just takes one piece of misinformation for people to run with,” Mackey says.
Misinformation: Repetition
Expert’s review
[The tweet about Gates and Fauci] was a pretty common theme. Repetition for this one is all about building an online campaign. Essentially propagation serves two roles: (1) getting [the fake message] out there that people who are against use of hydroxychloroquine are involved in a conspiracy to keep the treatment out of people’s hands; and (2) a campaign [to] force these public figures to actually get tested. — Tim Mackey, UC San Diego