Federal regulators have blocked two private sector enrollment websites from accessing consumer information through the federal Obamacare marketplace, citing “anomalous activity.”
The unusual step comes as the Centers for Medicare & Medicaid Services is under the gun to curb unauthorized enrollment and switching of Affordable Care Act plans by rogue agents. The agency received more than 200,000 complaints in the first six months of the year about such actions.
CMS said in a written statement that it had suspended the two sites — Benefitalign and Inshura — “while the anomalous activity is researched to ensure the EDE partners are in compliance with CMS data standards.” EDE stands for “enhanced direct enrollment” and refers to websites approved to integrate with healthcare.gov.
In a separate development, the two websites, which insurance brokers use instead of the federal healthcare.gov site to enroll clients in Affordable Care Act plans, are mentioned in an ongoing civil lawsuit filed by attorneys representing consumers and agents who claim they’ve been harmed by enrollment schemes.
CMS posted on Aug. 9 an updated list of websites approved to integrate with the federal Obamacare marketplace that no longer included Benefitalign and Inshura. As a result, insurance agents can’t use the websites to enroll customers in or make changes to their Obamacare plans.
Private sector enrollment sites were first allowed to integrate with healthcare.gov data under the Trump administration. About a dozen such sites are now approved to connect with the federal system.
Thwarting enrollment schemes and rogue insurance agents without making it too difficult for consumers and legitimate agents to enroll in health plans has become a political problem for the Biden administration. President Joe Biden has claimed record-breaking enrollment under the ACA as one of his administration’s major accomplishments.
In recent weeks, lawmakers have called on CMS to do more and introduced legislation to increase penalties for agents who enroll people in plans without authorization. The large number of complaints from victims of the schemes have caught the attention of House Republicans, who on June 28 requested investigations by the Government Accountability Office and the Office of Inspector General at the Department of Health and Human Services.
Subscribe to California Healthline’s free Daily Edition.
Until last month, agents using the approved private sector enrollment sites could access consumer information via healthcare.gov with only a name, birth date, and state of residence. CMS now requires three-way calls among agents, consumers, and the healthcare.gov helpline when agents new to a policy try to make a change. Many legitimate insurance agents are urging an additional fix used widely by state Obamacare enrollment systems: requiring two-factor authentication before consumer information can be accessed or changed by agents.
Meanwhile, the move to suspend the two enrollment websites baffled the companies, said Catherine Riedel, a spokesperson for TrueCoverage, an insurance call center that also does business as Inshura. TrueCoverage and Benefitalign are subsidiaries of Speridian Global Holdings of California.
“We don’t know what they want us to do differently,” she said.
The websites, she said, are cooperating with CMS, and they conducted an internal review that found no security issues. Very few details, other than “it is related to a potential technical anomaly reported by an outside party” were given, Riedel wrote, and the firms have not been provided “any specific, actionable information related to the alleged anomaly.”
Both firms are mentioned in the lawsuit first filed in April in the U.S. District Court for the Southern District of Florida. The suit alleges that people and organizations engaged in misleading advertising, or made changes to ACA policies, without the express permission of consumers — all with a goal of racking up commissions.
Late on Aug. 16, that case was amended to add allegations and defendants, including Benefitalign. The other enrollment website, Inshura, is not listed as a defendant, although it is run by TrueCoverage, which is.
Riedel said TrueCoverage disputes the lawsuit’s claims.
The case “is founded on misinformation and technical naivety that seems to have been connected to create a sensational and false narrative,” she said.
The Aug. 16 filing alleges that TrueCoverage or Speridian Technologies, another subsidiary of Speridian Global Holdings, used the Benefitalign or Inshura websites to access U.S. consumers’ personal information, then sent it to marketers in India and Pakistan. The allegation, if true, would violate agreements the private sector websites made with the federal government to gain approval to operate, the suit contends.
Riedel said there is no evidence to support the allegations and that it is technically impossible to move “bulk amounts of consumer data” from the Obamacare marketplace.
“Like many technology companies, some of TrueCoverage’s marketing efforts have been based in India. However, as part of that marketing work, TrueCoverage did not move any customer data out of the EDE platform,” she said.
The 185-page amended complaint added as a defendant Bain Capital Insurance Fund, part of one of the world’s leading private investment companies, saying it “aided and abetted” Florida-based Enhance Health, which describes itself as a large broker of ACA plans. Bain helped launch Enhance with a $150 million investment in 2021 and appointed its CEO.
After initially planning to market Medicare Advantage plans, the lawsuit says, Enhance Health and Bain decided to shift to ACA plans, which were seen as more profitable. The suit alleges Enhance Health participated in unauthorized agent changes or switching of ACA policies.
Bain knew “what was going on” at Enhance “and ultimately supported it,” the lawsuit says, noting that Bain executives sat on Enhance’s board, controlled the hiring of executives, and were often at its Sunrise, Florida, offices. The firm hoped to sell the company once it showed how profitable it could be, the suit alleges.
In a written statement, Enhance Health said that “upholding the highest standards of compliance and controls is a core focus in all aspects of our operation and we will vigorously defend against these baseless claims.”
Bain Capital Insurance did not reply to a request for comment.
The additional allegations expand on the initial April filing, which outlined a complex web of activities aimed at capitalizing changes to the ACA under Biden that resulted in broader availability of zero-premium plans for lower-income applicants. In some cases, consumers were lured to call centers through misleading ads touting nonexistent cash cards. Some call centers or agents filed duplicate coverage for the same individuals, without consumer permission, or split family members among multiple policies, the suit alleges.
Because the customers don’t pay monthly premiums for the plans, they may not notice they’ve been enrolled until they try to obtain care.
Some consumers whose plans were switched lost access to their doctors or medications. Some face tax consequences if they were enrolled in duplicative coverage or in subsidized plans for which they did not qualify.
One victim added to the case, Paula Langley of Texas, initially responded to an advertisement promising a cash card. She called the number advertised and was enrolled in ACA coverage in February 2023 but never received the promised incentive, according to the lawsuit.
She and her husband began receiving multiple insurance cards from different insurers, the suit says. She would show up for a doctor’s visit or to pick up a prescription only to find her coverage had been canceled, leaving her with unpaid medical bills.
All in all, she was switched among plans and agents at least 22 times in just over a year, the lawsuit alleges.
Attorneys Jason Kellogg of Miami and Jason Doss of Atlanta said they amended the lawsuit based on dozens of interviews with former employees of the named firms. They’re seeking class-action status on behalf of affected consumers and agents who have lost business to the unauthorized plan-switching, and the suit alleges violations of the federal Racketeer Influenced and Corrupt Organizations — or RICO — Act.
“The scheme is bad enough because it’s so large,” Kellogg said. “But it’s much worse given that it preys upon Americans who are at the lowest levels of the income scale, who may be desperate, are most vulnerable.”
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
SAVANNAH, Ga. — Blocks from where tourists stroll along the cobblestoned riverfront in this racially divided city, Detraya Gilliard made her way down the dark, ruptured sidewalks of Yamacraw Village, looking for her missing 15-year-old daughter.
Like most other people living in one of the nation’s oldest public housing projects, Gilliard endured the boarded-up buildings and mold-filled apartments because it was the only place she could afford.
Without working streetlights in parts of Yamacraw, Gilliard relied on the crescent moon’s glow to search for her daughter Desaray in May 2022. She passed yards dotted with clotheslines and power lines, and a broken-down playground littered with juice boxes and red Solo cups.
“I happened to look down, and I knew it was her by her feet, by the shoes she had on,” Gilliard said. She was “barely hanging on and she was covered in blood.”
The year before Desaray died, President Joe Biden called for the federal government to spend tens of billions of dollars to fix dilapidated public housing that he said posed “critical life-safety concerns.” The repairs, Biden said, would mostly help people of color, single mothers like Gilliard who work in low-income jobs, and people with disabilities.
The federal Department of Housing and Urban Development estimates that $115 billion is needed to fund a backlog of public housing repairs. But, two years ago, money to fund those repairs became a casualty of negotiations between the Biden administration and congressional lawmakers over the Inflation Reduction Act. Republicans also have blocked efforts to lift 25-year-old legislation that effectively prohibits the construction of additional public housing, despite the catastrophic public health consequences.
Yamacraw Village in Savannah, Georgia, is one of the nation’s oldest public housing projects. In 2022, Savannah’s city leaders unveiled Yamacraw Square, within the public housing complex, designed to pay tribute to the area’s African American and Native American history.(Renuka Rayasam/KFF Health News)
Tenants living in derelict housing face conditions that contribute to higher rates of heart disease, diabetes, asthma, violence, and other life-threatening risks.
The federal government has a long history of discriminatory practices in public housing. In cities across the country after World War II, Black families were barred from many public housing complexes even as the government induced white people to leave them by offering single-family homes in the suburbs subsidized by the Federal Housing Administration. Starting with the Nixon administration, lawmakers slowed investing in new public housing as more Black families and other people of color became tenants.
Today “residents are facing really terrible choices, or terrible options about their future,” said Sarah Saadian, senior vice president of policy for the National Low Income Housing Coalition. “We got here from Congress really failing to live up to its responsibilities of ensuring that people have access to an affordable, stable home.”
In 2022, an art deco luxury apartment building opened down the street. But little has changed in Yamacraw, which is filled with Black families.
Upscale condos and hotels surround Yamacraw Village, just a few blocks from Savannah’s tourist waterfront. (Renuka Rayasam/KFF Health News)
Current and former tenants say the Housing Authority of Savannah, the agency that oversees Yamacraw, has ignored the mold, rats, and roaches that infest the units and sicken residents, and the bullet holes in windows and gunshots that ring through the night. Now they fear the city is using the poor state of Yamacraw as justification to push residents out.
In April, an inspection of Yamacraw apartments conducted by HUD, which oversees taxpayer-supported public housing nationwide, found 29 “life-threatening” deficiencies that pose a high risk of death to residents, according to a preliminary report.
The inspection cited 28 deficiencies it called “severe,” meaning they present a high risk of permanent disability, serious injury, or illness. An additional 195 deficiencies were cited as “moderate” because they could cause temporary harm or prompt a visit to a doctor.
Research links structural racism and disinvestment to chronic gun violence, which has taken a heavy toll on Black neighborhoods and kids such as Desaray. A study of gun injuries in four large cities at the height of the covid-19 pandemic found that Black children were 100 times as likely as white youths to suffer a firearm assault.
Desaray Gilliard was a freshman in high school when she died in May 2022, while living in one of the nation’s oldest public housing projects, in Savannah, Georgia. The teen’s shooting death at Yamacraw Village remains unsolved.(Detraya Gilliard)
Study co-author Jonathan Jay, an assistant professor of community health sciences at Boston University, saidmost of the country’s gun violence stems from disputes in neighborhoods that lack investment in housing and other public services
“This is about white privilege,” Jay said. “The result is driven by racist policymaking.”
Desaray Gilliard was a high school freshman when she was killed. She loved clothes, music, dancing, and the color pink, her mother said. She planned to go to Italy with her art class. She was excited about learning to drive and getting a job. Desaray had her sights set on attending Ohio State University.
They’d lived in Yamacraw for seven years. The teen’s shooting death remains unsolved.
Gilliard has struggled with thoughts of self-harm, she said. She maintains a memorial with pictures, stuffed animals, and flowers near the spot where she found Desaray’s body.
“I have to remember this is for her,” she said of her middle child’s death, “because nobody else is doing these things for her to keep her memory alive.”
A Broken Promise?
Federally funded public housing must be kept in “decent, safe and sanitary” condition, according to HUD. In 2013, the agency’s then secretary, Shaun Donovan, visited Savannah to announce a program that could give the local housing authority millions of dollars to rehab four public housing complexes, including Yamacraw, which has been among the lowest-rated public housing complexes in Georgia.
The Rental Assistance Demonstration program touted by Donovan did not provide new public money. Instead, it loosened rules to allow local officials to work with private lenders and developers to pay for repairs, transforming public housing complexes into mixed-income developments with Section 8 project-based rental assistance.
Last year, a consultants’ report found a host of problems in Yamacraw, including water leaks and faulty wiring. “The Remaining Useful Life of the Property is estimated to be 0 years,” the consultants wrote. The housing authority wants to demolish Yamacraw and replace it with homes that are “healthier, more energy efficient and accessible,” the report said.
After her daughter didn’t return home one night in May 2022, Detraya Gilliard went looking for her. She waited for about 30 minutes at a bench near a park in the middle of the complex, hoping her daughter would find her.(Renuka Rayasam/KFF Health News)
Yamacraw never saw the windfall Donovan promised, current and former tenants said. Even with a housing assistance waitlist of more than 3,000 families in Savannah, records show most of the 315 apartments in Yamacraw sit empty, many with boarded-up doors and windows. Some other public housing developments in the area have been repaired or rebuilt, but except for new roofing added in 2019, Yamacraw has not had a significant renovation in years, according to the consultants’ report.
Rather than repair the units, local officials started a process to tear down the complex, threatening to displace residents who have nowhere else to go in a city where the average two-bedroom apartment rents for more than $1,600 monthly.
Congress has provided less money than was needed over the past 20 years to fix Yamacraw and other public housing complexes nationwide, leaving local agencies in a tough spot, said Earline Davis, executive director of the Housing Authority of Savannah.
The housing authority still plans to demolish Yamacraw and redevelop the property with new affordable housing, she said. Residents fear that they will be pushed out, and that because of its prime location, the redevelopment plans would prioritize apartments that attract people who can afford higher rents.
Georgia Benton grew up in Yamacraw Village. She and her son, LaRay Benton, have been fighting the housing authority’s current redevelopment plans. They say the plans would displace residents and disrupt the two-century-old First Bryan Baptist Church.(Renuka Rayasam/KFF Health News)
“Anytime you want to do something to make money — go destroy the historic Black community,” said Georgia Benton, who grew up in Yamacraw. “But ain’t nobody hollerin’ ‘Stop.’”
She and her son LaRay Benton have been fighting the housing authority’s redevelopment plans, which they say could also disrupt the two-century-old First Bryan Baptist Church. Rev. Andrew Bryan, a former enslaved person and ordained minister, founded the church in 1788. He later bought his freedom.
The Bentons and three City Council members went door to door observing the condition of residents’ units. They said plumbing issues caused sewage overflows and leaky faucets, mold tracked across the ceilings, and there were insect and rodent infestations.
Many families said they developed respiratory problems, such as bronchitis and asthma, after they moved in. “It is an unhealthy situation,” LaRay Benton said.
The two-century-old First Bryan Baptist Church is part of the Yamacraw Village community. It was founded in 1788 by the Rev. Andrew Bryan, a former enslaved person and ordained minister who later bought his freedom.(Renuka Rayasam/KFF Health News)
About seven years ago, after his previous Savannah landlord raised the rent, Paris Snead, his wife, and two children found themselves homeless. A nonprofit helped them get into Yamacraw, where rent was $750 a month.
It’s been years since they left. Snead said he still takes a daily allergy pill because he believes he was exposed to mold in his unit, which caused allergy-like symptoms.
“The walls sweat like working men,” Snead said of his former apartment. “The walls will, literally, from the top to the bottom, leak water.”
“When you’re homeless, and you want to be able to have a place for your kids, I mean, you’ll make a home wherever you can,” he said.
Snead said he showed Yamacraw’s management the leaking walls, but they didn’t act.
Subscribe to California Healthline’s free Daily Edition.
“The management team there did more to evict people and cause problems than they did to help families and ensure they had a place to stay,” Snead said.
HUD, which conducts periodic inspections at public housing complexes, declined an interview request. The agency referred questions to the Housing Authority of Savannah.
The housing authority’s redevelopment plans have been delayed by HUD’s lengthy approval process, said Savannah Mayor Van R. Johnson II, who appoints people to a five-member board of commissioners that helps oversee the city’s public housing.
He said he met with HUD acting Secretary Adrianne Todman and other HUD officials about housing issues in Savannah.
“People don’t deserve to live like that,” Johnson said.
If Yamacraw is demolished and rebuilt, he said, current tenants will have a chance to return because the homes will be affordable to people with low incomes.
Nobody else is doing these things for her to keep her memory alive.
Detraya Gilliard
‘The Worst Experience of My Life’
Yamacraw’s struggles are rooted in century-old policies that have made it difficult for many Black neighborhoods to thrive.
In the 1930s, the federal government’s Home Owners’ Loan Corp. made color-coded maps for Savannah and 238 other cities and labeled redlined areas — usually places where Black people, Jews, immigrants, and Catholics lived — as undesirable for investment.
“The houses are occupied by the lowest class negro tenants,” a government surveyor wrote.
Yamacraw was opened in 1941 as segregated public housing for Black people. Today a health clinic occupies the original administrative building, designed to look like a plantation house.
Despite its problems, Johnson said, some of the city’s most prominent doctors, lawyers, and ministers grew up in Yamacraw.
Records show most of the 315 apartments in Yamacraw Village sit empty, many with boarded-up doors and windows. (Renuka Rayasam/KFF Health News)
Former and current tenants said the apartments slowly descended into disrepair.
Some lawmakers have used the poor state of public housing as justification to refuse lifting a moratorium passed during the Clinton administration that prohibits the construction of additional units, even as the nation’s rental prices — and evictions — soar.
The argument that public housing “doesn’t work” is disingenuous, said Saadian, with the National Low Income Housing Coalition.
“The federal government really failed to invest in public housing, to keep it in good condition, and to keep those communities thriving,” Saadian said, “and in many cases, actively contributed to those communities declining.”
Instead of repairing public housing and building more high-quality units, federal lawmakers promised to provide housing vouchers, commonly known as Section 8, which helps people with low incomes rent privately owned homes. But most people who qualify for vouchers never receive them. Those who do often struggle to find landlords who will accept them, rendering them sometimes worthless.
Without working streetlights in parts of Yamacraw Village, Detraya Gilliard had only the crescent moon’s glow to search for her daughter Desaray in May 2022. She passed yards dotted with clotheslines and power lines, and a broken-down playground littered with juice boxes and red Solo cups.(Renuka Rayasam/KFF Health News)
Three years ago, LaTonya Atterbury was living in hotels north of Atlanta when she was offered a unit in Yamacraw for $511 a month. In August 2021, she moved in with her niece, now 29, and her niece’s son, now 8, relieved to have more stable housing.
But within the first week, she said, a neighbor’s son broke her window and the housing authority charged her $60 to fix it. She said her bathroom is covered in mold and mildew. One day, months after she moved in, Atterbury noticed a hole in her second-story window and saw a bullet on the floor, and realized there had been a shooting overnight. No one was injured, she said, but the bullet hole was only recently fixed — about 2½ years after the incident.
“It’s been the worst experience of my life,” Atterbury said. “Sitting here will make you very depressed.”
Atterbury said she and other residents remain in Yamacraw at least in part because the housing authority has promised vouchers to move elsewhere. Three years later, she is still waiting.
Demolishing and rebuilding Yamacraw could take years.
Davis, the housing authority’s executive director, said her agency has repeatedly told tenants they would be relocated to other public housing complexes or given a Section 8 voucher during construction if they have no lease violations. But residents say they routinely receive lease violations for harmless acts such as broken blinds. LaRay Benton said one resident was cited and fined $75 for leaving a stroller on her front porch while she took her baby inside.
Yamacraw Village, one of the nation’s oldest public housing projects, sits just blocks from Savannah’s tourist riverfront.(Renuka Rayasam/KFF Health News)
A Mother’s Search
Researchers said that the presence of abandoned buildings can contribute to violent crime by making people feel unsafe and creating a sense of disorder. Studies suggest that razing abandoned buildings and improving green space can reduce it.
“No gun policy is going to work if we don’t fix social infrastructure,” said Jonathan Metzl, director of the Department of Medicine, Health, and Society at Vanderbilt University. “We need investments to make sure communities feel safe. This is not just a public health problem. This is a race problem. This is a democracy problem.”
In recent years, shooting victims or their relatives, including Desaray’s mother, have filed at least three lawsuits against the Housing Authority of Savannah. Those ongoing lawsuits allege the agency failed to take added security measures in its public housing complexes — some of which had fallen into disrepair — despite gun violence and other crimes.
“I don’t know how we can prevent shootings,” Davis said.
Davis declined to comment on the lawsuits. She would say only that her agency has installed cameras in Yamacraw, worked with police, and asked residents to report crime. The actions came after Desaray’s death.
Johnson, Savannah’s mayor, said police have investigated the Desaray Gilliard case, but there are people “who know what happened” and will not talk to officers.
Detraya Gilliard maintains a memorial with pictures, stuffed animals, and flowers near the spot where she found Desaray’s body, but her visits to Yamacraw Village are traumatic.(Bobby Williams)
Around 9 p.m. on a Friday night two years ago, Gilliard went looking for her daughter for the second time that night. Desaray missed an 8 p.m. curfew and wasn’t answering her phone.
Gilliard waited for about 30 minutes at a bench near a park in the middle of the complex, hoping Desaray would find her. Then she started to retrace her steps.
Gilliard called 911 after she saw her daughter’s body.
When the police arrived, they made their way through the darkened complex with flashlights, Gilliard said. An officer pulled up Desaray’s shirt and saw a bullet hole in her chest. Gilliard said she later learned from a funeral director that her daughter had been shot three times. She has yet to receive an autopsy report from the police.
Gilliard said “nothing has changed before, since, or after” her daughter’s death.
“It’s been very difficult,” she said. “Sometimes I wanted to give up. I even thought about committing suicide.”
About a month after Desaray died, Gilliard said someone tried to break into her apartment. A couple of weeks later, her request to move to a new complex was finally granted and Gilliard left Yamacraw.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
The rapidly evolving field of street medicine — the practice of providing health care to homeless people living outside — is getting a jolt in California with a new player: a medical group devoted exclusively to homeless people.
And it’s actually making money.
Sachin Jain, who worked on federal Medicaid policy during his tenure in the Obama administration, helped spearhead a Southern California-based street medicine group called Healthcare in Action in 2021 — and makes no bones about wanting to capture new money from the state and federal governments to treat and house homeless people.
“Health-care issues cause homelessness, but they are also exacerbated by homelessness,” Jain told me. “And the dollars in health care are enormous.”
Around the country, Jain and street medicine doctors and nurses — who have long practiced on the fringes of the health-care system with little revenue — are becoming integral players in the Biden administration’s effort to address the consequences of homelessness.
No longer reliant on inconsistent funding and charitable giving, many street medicine operations are taking advantage of billions in Medicaid dollars to provide social services, from helping patients find an apartment to paying their utility bills. Since October, the federal government has also boosted reimbursements for providers caring for homeless people in the field.
“We’re being brought into the insurance world, and we’re eligible for reimbursement now,” said Jim Withers, a longtime street medicine provider in Pittsburgh who helped start the movement. “We’re legit!”
But Withers is wary of the moneymaking endeavors popping up to treat homeless people.
“I do worry about the corporatization of street medicine and capitalism invading what we’ve been building,” he said. “Caring for people under bridges and on the streets does not always align with the economics of our health-care system. The spirit of the street medicine movement has been one of social justice, but nobody owns the streets.”
California is an ideal laboratory for this new world of Medicaid-funded social services. It is home to more people living on streets and sidewalks, in vehicles, or along waterways than any other state. It is also home to more street medicine providers than anywhere else: 64 of the roughly 150 street medicine organizations across the country are here.
Healthcare in Action employs doctors, nurses and social workers who deliver a range of medical services, including basic wound care, medication administration and antipsychotic injections.
Its street medicine teams operate in 17 California communities and revenue are soaring, reaching $15.4 million in 2023, up from $2 million in 2021. It makes money from Medicaid and charitable contributions, among other sources. It also contracts with hospitals, health insurance companies and municipalities to provide services.
Jain says Healthcare in Action addresses sickness on the streets and saves the health system money by keeping homeless people with costly conditions out of hospitals and jails.
His street medicine teams also work to get people food, addiction treatment and, in some cases, housing.
But much of the teams’ time and energy is dedicated to building trust. It can take time to persuade people to agree to medical care, or housing, for that matter.
“One of the challenges in health care is we dehumanize people who experience homelessness,” Jain said. “We see them as not as worthy of the courtesies that the rest of us have.”
This article is not available for syndication due to republishing restrictions. If you have questions about the availability of this or other content for republication, please contact [email protected].
Jamie Holmes says a surgery center tried to make her pay for two operations after she underwent only one. She refused to buckle, even after a collection agency sued her last winter.
Holmes, who lives in northwestern Washington state, had surgery in 2019 to have her fallopian tubes tied, a permanent birth-control procedure that her insurance company agreed ahead of time to cover.
During the operation, while Holmes was under anesthesia, the surgeon noticed early signs of endometriosis, a common condition in which fibrous scar tissue grows around the uterus, Holmes said. She said the surgeon later told her he spent about 15 minutes cauterizing the troublesome tissue as a precaution. She recalls him saying he finished the whole operation within the 60 minutes that had been allotted for the tubal ligation procedure alone.
She said the doctor assured her the extra treatment for endometriosis would cost her little, if anything.
Then the bill came.
The Patient: Jamie Holmes, 38, of Lynden, Washington, who was insured by Premera Blue Cross at the time.
Medical Services: A tubal ligation operation, plus treatment of endometriosis found during the surgery.
Service Provider: Pacific Rim Outpatient Surgery Center of Bellingham, Washington, which has since been purchased, closed, and reopened under a new name.
Total Bill: $9,620. Insurance paid $1,262 to the in-network center. After adjusting for prices allowed under the insurer’s contract, the center billed Holmes $2,605. A collection agency later acquired the debt and sued her for $3,792.19, including interest and fees.
What Gives: The surgery center, which provided the facility and support staff for her operation, sent a bill suggesting that Holmes underwent two separate operations, one to have her tubes tied and one to treat endometriosis. It charged $4,810 for each.
Subscribe to California Healthline’s free Daily Edition.
Holmes said there were no such problems with the separate bills from the surgeon and anesthesiologist, which the insurer paid.
Holmes figured someone in the center’s billing department mistakenly thought she’d been on the operating table twice. She said she tried to explain it to the staff, to no avail.
She said it was as if she ordered a meal at a fast-food restaurant, was given extra fries, and then was charged for two whole meals. “I didn’t get the extra burger and drink and a toy,” she joked.
Her insurer, Premera Blue Cross, declined to pay for two operations, she said. The surgery center billed Holmes for much of the difference. She refused to pay.
Holmes said she understands the surgery center could have incurred additional costs for the approximately 15 minutes the surgeon spent cauterizing the spots of endometriosis. About $500 would have seemed like a fair charge to her. “I’m not opposed to paying for that,” she said. “I am opposed to paying for a whole bunch of things I didn’t receive.”
Holmes figured it was a mistake when she was billed for two surgeries after being on the operating table just once. Her insurer, Premera Blue Cross, declined to pay for two operations, she says. The surgery center billed Holmes for much of the difference.(Ting-Li Wang for KFF Health News)
The physician-owned surgery center was later purchased and closed by PeaceHealth, a regional health system. But the debt was turned over to a collection agency, SB&C, which filed suit against Holmes in December 2023, seeking $3,792.19, including interest and fees.
The collection agency asked a judge to grant summary judgment, which could have allowed the company to garnish wages from Holmes’ job as a graphic artist and marketing specialist for real estate agents.
Holmes said she filed a written response, then showed up on Zoom and at the courthouse for two hearings, during which she explained her side, without bringing a lawyer. The judge ruled in February that the collection agency was not entitled to summary judgment, because the facts of the case were in dispute.
Representatives of the collection agency and the defunct surgery center declined to comment for this article.
Sabrina Corlette, co-director of Georgetown University’s Center on Health Insurance Reforms, said it was absurd for the surgery center to bill for two operations and then refuse to back down when the situation was explained. “It’s like a Kafka novel,” she said.
Corlette said surgery center staffers should be accustomed to such scenarios. “It is quite common, I would think, for a surgeon to look inside somebody and say, ‘Oh, there’s this other thing going on. I’m going to deal with it while I’ve got the patient on the operating table.’”
It wouldn’t have made medical or financial sense for the surgeon to make Holmes undergo a separate operation for the secondary issue, she said.
Corlette said that if the surgery center was still in business, she would advise the patient to file a complaint with state regulators.
The Resolution: So far, the collection agency has not pressed ahead with its lawsuit by seeking a trial after the judge’s ruling. Holmes said that if the agency continues to sue her over the debt, she might hire a lawyer and sue them back, seeking damages and attorney fees.
She could have arranged to pay off the amount in installments. But she’s standing on principle, she said.
“I just got stonewalled so badly. They treated me like an idiot,” she said. “If they’re going to be petty to me, I’m willing to be petty right back.”
The Takeaway: Don’t be afraid to fight a bogus medical bill, even if the dispute goes to court.
Debt collectors often seek summary judgment, which allows them to garnish wages or take other measures to seize money without going to the trouble of proving in a trial that they are entitled to payments. If the consumers being sued don’t show up to tell their side in court hearings, judges often grant summary judgment to the debt collectors.
However, if the facts of a case are in dispute — for example, because the defendant shows up and argues she owes for just one surgery, not two — the judge may deny summary judgment and send the case to trial. That forces the debt collector to choose: spend more time and money pursuing the debt or drop it.
“You know what? It pays to be stubborn in situations like this,” said Berneta Haynes, a senior attorney for the National Consumer Law Center who reviewed Holmes’ bill for California Healthline.
Many people don’t go to such hearings, sometimes because they didn’t get enough notice, don’t read English, or don’t have time, she said.
“I think a lot of folks just cave” after they’re sued, Haynes said.
Holmes says she tried to explain her situation to the surgery center’s staff, to no avail — then refused to back down when she was sued for the debt. “I just got stonewalled so badly. They treated me like an idiot,” she says. “If they’re going to be petty to me, I’m willing to be petty right back.”(Ting-Li Wang for KFF Health News)
Emily Siner reported the audio story.
After six years, we’ll have a final installment with NPR of our Bill of the Month project in the fall. But Bill of the Month will continue at KFF Health News and elsewhere. We still want to hear about your confusing or outrageous medical bills. Visit Bill of the Month to share your story.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
SAN FRANCISCO — For years, Latinos represented the biggest share of new HIV cases in this city, but testing data suggests the tide may be turning.
The number of Latinos newly testing positive for HIV dropped 46% from 2022 to 2023, according to a preliminary report released in July by the San Francisco Department of Public Health.
The decrease could mark the first time in five years that Latinos haven’t accounted for the largest number of new cases, leading to cautious optimism that the millions of dollars the city has spent to remedy the troubling disparity is working. But outreach workers and health care providers say that work still needs to be done to prevent, and to test, for HIV, especially among new immigrants.
“I am very hopeful, but that doesn’t mean that we’re going to let up in any way on our efforts,” said Stephanie Cohen, who oversees the city’s HIV program.
Public health experts said the city’s latest report could be encouraging, but that more data is needed to know whether San Francisco has addressed inequities in its HIV services. For instance, it’s still unclear how many Latinos were tested or if the number of Latinos exposed to the virus had also fallen — key health metrics the public health department declined to provide to California Healthline. Testing rates are also below pre-pandemic levels, according to the city.
“If there are fewer Latinos being reached by testing efforts despite a need, that points to a serious challenge to addressing HIV,” said Lindsey Dawson, the associate director of HIV Policy and director of LGBTQ Health Policy at KFF, a health information nonprofit that includes California Healthline.
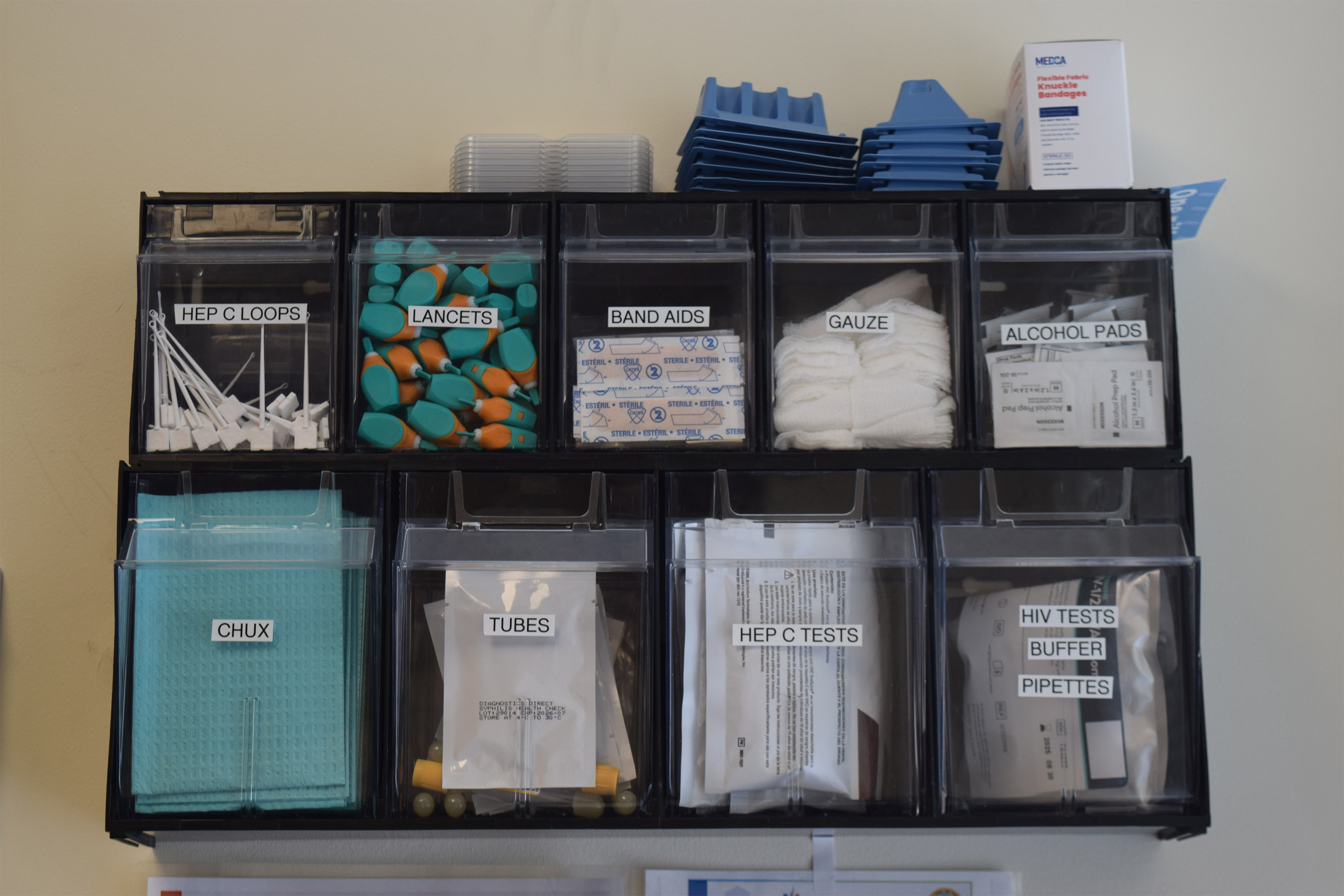
The center of the HIV epidemic in the mid-1980s, San Francisco set a national model for response to the disease after building a network of HIV services for residents to get free or low-cost HIV testing, as well as treatment, regardless of health insurance or immigration status. (Vanessa G. Sánchez/KFF Health News)
San Francisco provides free testing for infectious diseases, but outreach workers say many new immigrants still do not know where to get testing or they often have a difficult time navigating the health care system. (Vanessa G. Sánchez/KFF Health News)
Contreras reaches for a bin containing condoms during an outreach event in the Tenderloin neighborhood of San Francisco.(Vanessa G. Sánchez/KFF Health News)
San Francisco, like the rest of the country, suffers major disparities in diagnosis rates for Latinos and people of color. Outreach workers say that recent immigrants are more vulnerable to infectious diseases because they don’t know where to get tested or have a hard time navigating the health care system.
In 2022, Latinos represented 44% of new HIV cases in San Francisco, even though they accounted for only 15% of the population. Latinos’ share of new cases fell to 30% last year, while whites accounted for the largest share of new cases at 36%, according to the new report.
Cohen acknowledged a one-year decline is not enough to draw a trend, but she said targeted funding to community-based organizations may have helped lower HIV cases among Latinos. A final report is expected in the fall.
Most cities primarily depend on federal dollars to pay for HIV services, but San Francisco has an ambitious target to be the first U.S. city to eliminate HIV, and roughly half of its $44 million HIV/AIDS budget last year came from city coffers. By comparison, New Orleans, which has similar HIV rates, kicked in only $22,000 of its $13 million overall HIV/AIDS budget, according to that city’s health department.
As part of an effort to address HIV disparities among LGBTQ+ communities and people of color, San Francisco last year gave $2.1 million to three nonprofits — Instituto Familiar de la Raza, Mission Neighborhood Health Center, and San Francisco AIDS Foundation — to bolster outreach, testing, and treatment among Latinos, according to the city’s 2023 budget.
At Instituto Familiar de la Raza, which administers the contract, the funding has helped pay for HIV testing, prevention, treatment, outreach events, counseling, and immigration legal services, said Claudia Cabrera-Lara, director of the HIV program at Sí a la Vida. But ongoing funding isn’t guaranteed.
“We live with the anxiety of not knowing what is going to happen,” she said.
Subscribe to California Healthline’s free Daily Edition.
The public health department has commissioned a $150,000 project with Instituto Familiar de la Raza to determine how Latinos are contracting HIV, who is most at risk, and what health gaps remain. The results are expected in September.
“It could help us shape, pivot, and grow our programs in a way that makes them as effective as possible,” Cohen said.
The center of the HIV epidemic in the mid-1980s, San Francisco set a national model for response to the disease after building a network of HIV services for residents to get free or low-cost HIV testing, as well as treatment, regardless of health insurance or immigration status.
Although city testing data showed that new cases among Latinos declined last year, outreach workers are seeing the opposite. They say they are encountering more Latinos diagnosed with HIV while they struggle to get out information about testing and prevention — such as taking preventive medications like PrEP — especially among the young and gay immigrant communities.
San Francisco’s 2022 epidemiological data shows that 95 of the 213 people diagnosed at an advanced stage of the virus were foreign-born. And the diagnosis rate among Latino men was four times as high as the rate for white men, and 1.2 times that of Black men.
“It’s a tragedy,” said Carina Marquez, associate professor of medicine in the Division of HIV, Infectious Diseases, and Global Medicine at Zuckerberg San Francisco General Hospital, the city’s largest provider of HIV care. “We have such great tools to prevent HIV and to treat HIV, but we are seeing this big disparity.”
Because Latinos are the ethnicity least likely to receive care in San Francisco, outreach workers want the city to increase funding to continue to reduce HIV disparities.
The San Francisco AIDS Foundation, for instance, would like more bilingual sexual health outreach workers; it currently has four, to cover areas where Latinos have recently settled, said Jorge Zepeda, its director of Latine Health Services.
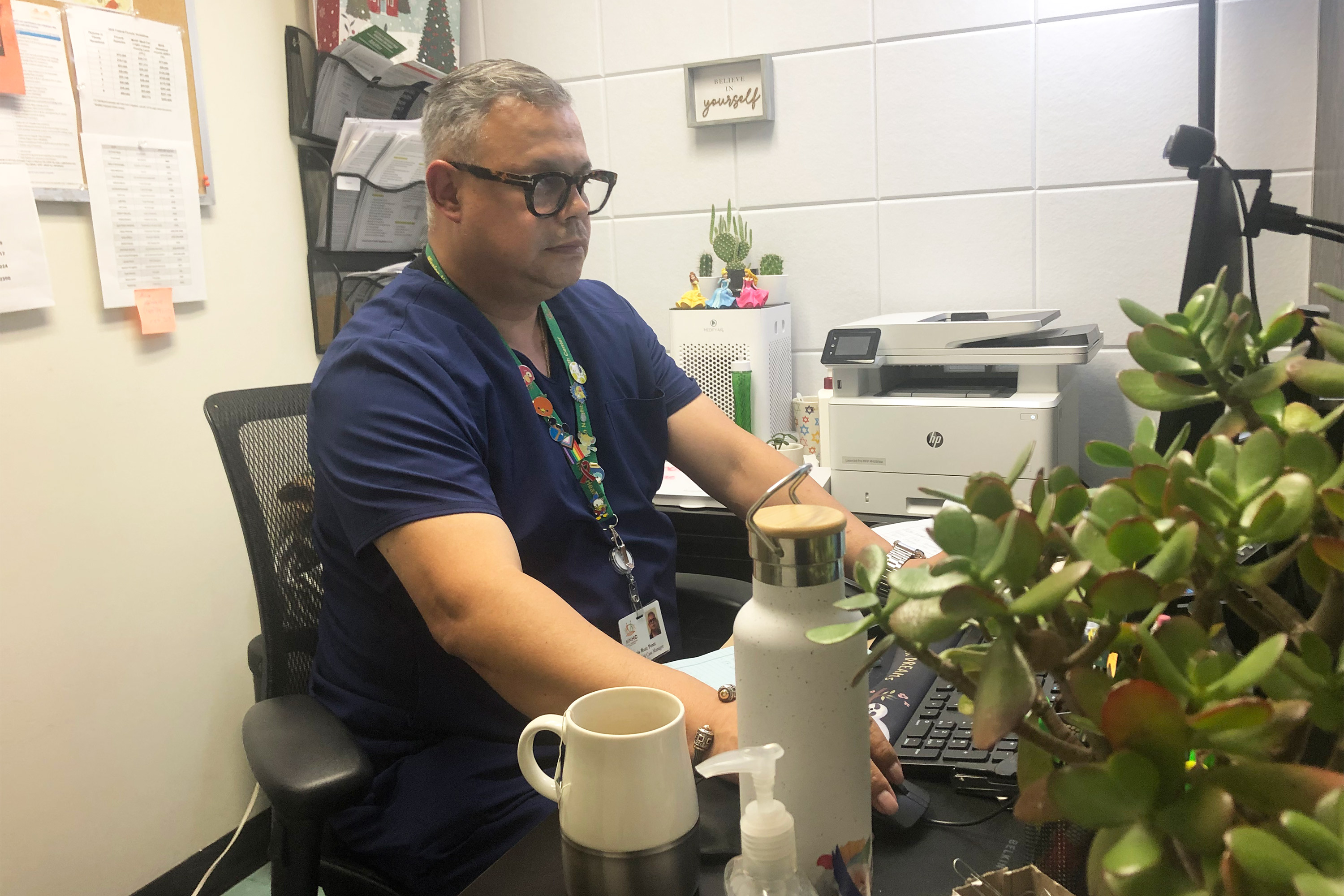
Luis Carlos Ruiz Perez, an HIV medical case manager, says it’s a challenge to connect Latinos to bilingual services for mental health and substance abuse, something that is crucial to maintaining their HIV care. (Vanessa G. Sánchez/KFF Health News)
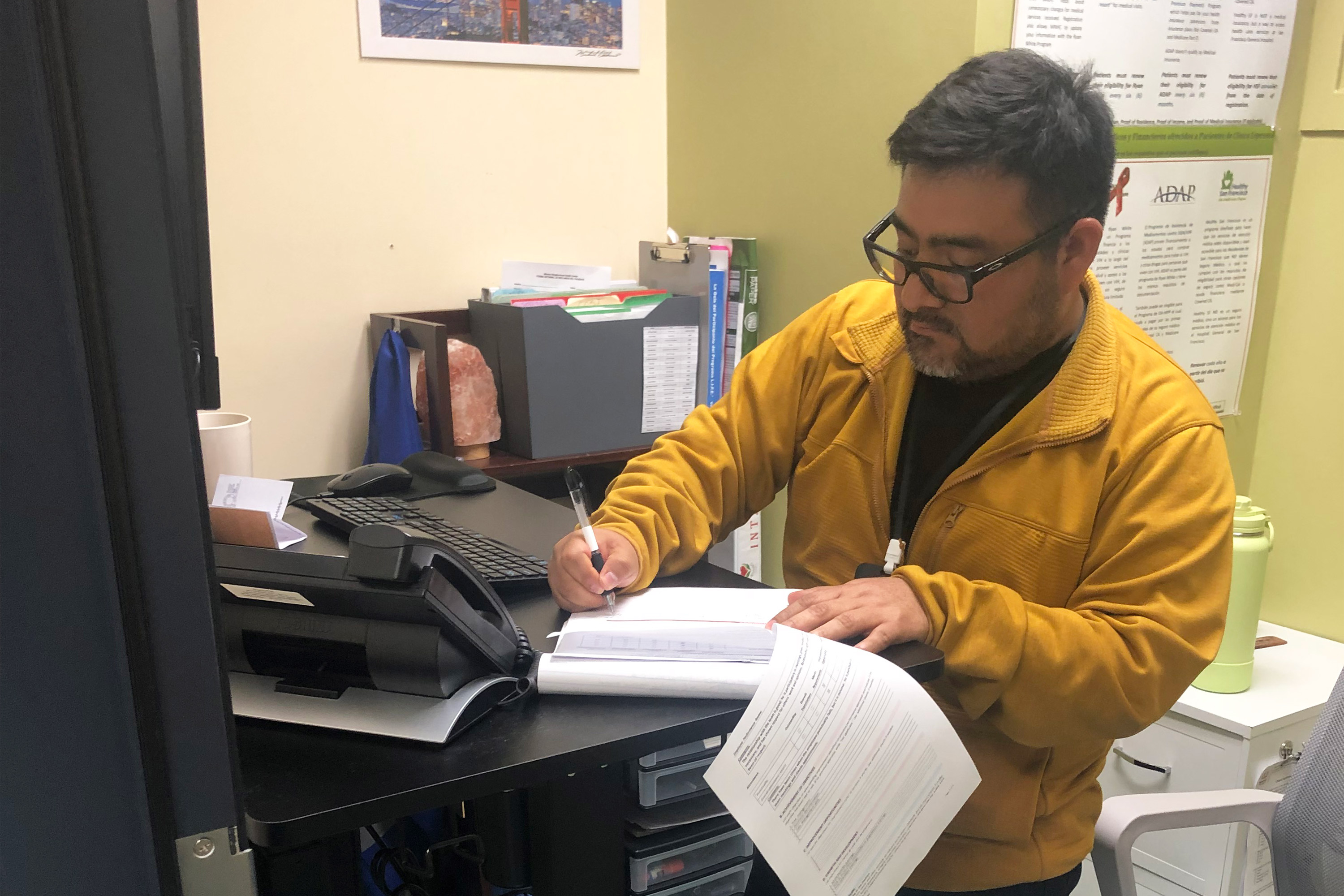
Ivan Ramirez, HIV services supervisor at Clinica Esperanza, says the number of people seeking HIV treatment has jumped from about two a month to an average of about 16 a month at his clinic in the Mission District of San Francisco. (Vanessa G. Sánchez/KFF Health News)
At Mission Neighborhood Health Center, which runs Clinica Esperanza, one of the largest providers of HIV care to Latinos and immigrants, the number of patients seeking treatment has jumped from about two a month to around 16 a month.
Among the challenges is getting patients connected to mental health and substance abuse bilingual services crucial to retaining them in HIV care, said Luis Carlos Ruiz Perez, the clinic’s HIV medical case manager. The clinic wants to advertise its testing and treatment services more but lacks the money.
“A lot of people don’t know what resources are available. Period,” said Liz Oates, a health systems navigator from Glide Foundation, who works on HIV prevention and testing. “So where do you start when nobody’s engaging you?”
Newswise — Irvine, Calif., Aug. 20, 2024 — A team of researchers led by the University of California, Irvine has discovered that an antioxidant found in rosemary extract can reduce volitional intakes of cocaine by moderating the brain’s reward response, offering a new therapeutic target for treating addiction.
The study, recently published online in the journal Neuron, describes team members’ focus on a region of the brain called the globus pallidus externus, which acts as a gatekeeper that regulates how we react to cocaine. They discovered that within the GPe, parvalbumin-positive neurons are crucial in controlling the response to cocaine by changing the activity neurons releasing the pleasure molecule dopamine.
“There are currently no effective therapeutics for dependence on psychostimulants such as cocaine, which, along with opioids, represent a substantial health burden,” said corresponding author Kevin Beier, UC Irvine associate professor of physiology and biophysics. “Our study deepens our understanding of the basic brain mechanisms that increase vulnerability to substance use disorder-related outcomes and provides a foundation for the development of new interventions.”
Findings in mice revealed that globus pallidus externus parvalbumin-positive cells, which indirectly influence the release of dopamine, become more excitable after being exposed to cocaine. This caused a drop in the expression of certain proteins that encode membrane channels that usually help keep the globus pallidus cell activity in check. Researchers found that carnosic acid, an isolate of rosemary extract, selectively binds to the affected channels, providing an avenue to reduce response to the drug in a relatively specific fashion.
“Only a subset of individuals are vulnerable to developing a substance use disorder, but we cannot yet identify who they are. If globus pallidus cell activity can effectively predict response to cocaine, it could be used to measure likely responses and thus serve as a biomarker for the most vulnerable,” Beier said. “Furthermore, it’s possible that carnosic acid could be given to those at high risk to reduce the response to cocaine.”
The next steps in this research include thoroughly assessing negative side effects of carnosic acid and determining the ideal dosage and timing. The team is also interested in testing its efficacy in reducing the desire for other drugs and in developing more potent and targeted variants.
In addition to UC Irvine researchers, scientists from the University of West Virginia and the University of Colorado participated in the study. See the full list here.
This work was supported by grants from the National Institutes of Health, One Mind, the Alzheimer’s Association, New Vision Research, BrightFocus Foundation, and the Brain & Behavior Research Foundation.
About the University of California, Irvine: Founded in 1965, UC Irvine is a member of the prestigious Association of American Universities and is ranked among the nation’s top 10 public universities by U.S. News & World Report. The campus has produced five Nobel laureates and is known for its academic achievement, premier research, innovation and anteater mascot. Led by Chancellor Howard Gillman, UC Irvine has more than 36,000 students and offers 224 degree programs. It’s located in one of the world’s safest and most economically vibrant communities and is Orange County’s second-largest employer, contributing $7 billion annually to the local economy and $8 billion statewide. For more on UC Irvine, visit www.uci.edu.
Media access: Radio programs/stations may, for a fee, use an on-campus studio with a Comrex IP audio codec to interview UC Irvine faculty and experts, subject to availability and university approval. For more UC Irvine news, visit news.uci.edu. Additional resources for journalists may be found at https://news.uci.edu/media-resources.
En los 18 meses posteriores a ser diagnosticada con la reaparición de un cáncer de ovarios que creía haber superado hace 20 años, Francine Milano viajó dos veces desde su casa de Pennsylvania a Vermont. No fue a esquiar, ni a hacer senderismo, ni a disfrutar del paisaje, sino a organizar su muerte.
“Quería tener el control sobre cómo iba a dejar este mundo”, dijo la mujer de 61 años que vive en Lancaster. “Decidí que era algo que yo podía elegir”.
Usar asistencia médica para morir no fue una opción cuando Milano supo, a principios de 2023, que su enfermedad era incurable. En ese momento, habría tenido que viajar a Suiza, o vivir en el Distrito de Columbia o en uno de los 10 estados donde la muerte asistida era legal.
Pero Vermont eliminó su requisito de residencia en mayo de 2023, seguido de Oregon dos meses después. (Montana permite la muerte asistida en virtud de una decisión judicial de 2009, pero ese fallo no establece normas sobre la residencia. Y aunque Nueva York y California consideraron recientemente una legislación que permitiría a los residentes fuera del estado acceder a la ayuda médica para morir, ninguna de las dos disposiciones fue aprobada).
A pesar de las limitadas opciones y los retos —como encontrar médicos en un nuevo estado, decidir dónde morir y viajar cuando se está demasiado enfermo para caminar hasta el dormitorio o para subirse a un coche— docenas de personas han hecho el viaje a los dos estados que han abierto sus puertas a los enfermos terminales no residentes que buscan ayuda para morir.
Al menos 26 personas han viajado a Vermont para morir, lo que representa casi el 25% de las muertes asistidas registradas en el estado desde mayo de 2023 hasta junio de 2024, según el Departamento de Salud de Vermont. En Oregon, 23 residentes de fuera del estado murieron utilizando asistencia médica en 2023, algo más del 6% del total del estado, según la Autoridad de Salud de Oregon.
El oncólogo Charles Blanke, cuya clínica en Portland se especializa en la atención al final de la vida, señaló que el total de Oregon es probablemente el resultado de un recuento inexacto y espera que las cifras aumenten. En el último año, dijo, ha atendido de dos a cuatro pacientes de fuera del estado a la semana —aproximadamente una cuarta parte de su consulta— y ha recibido llamadas de todo el país, incluyendo Nueva York, las Carolinas, Florida y “toneladas de Texas”. Pero que los pacientes estén dispuestos a viajar no significa que sea fácil ni que obtengan el resultado deseado.
“La ley es muy estricta sobre lo que hay que hacer”, afirmó Blanke.
Como en otros estados que permiten lo que algunos llaman muerte asistida por un médico o suicidio asistido, Oregon y Vermont exigen que los pacientes sean evaluados por dos médicos.
Los pacientes deben tener menos de seis meses de vida, estar mental y cognitivamente sanos, y ser físicamente capaces de tomar los fármacos para poner fin a sus vidas. Los historiales deben revisarse en el estado; no hacerlo constituye ejercer la medicina fuera del estado, lo que infringe los requisitos para obtener la licencia médica.
Por la misma razón, los pacientes deben estar en el estado para el examen inicial, cuando solicitan los fármacos y cuando los toman.
Las legislaturas estatales imponen esas restricciones como salvaguardias, para equilibrar los derechos de los pacientes que solicitan ayuda para morir con el imperativo legislativo de no aprobar leyes que puedan perjudicar a las personas, explicó Peg Sandeen, CEO del grupo Death With Dignity (Muerte con Dignidad). Sin embargo, al igual que muchos defensores de la muerte asistida, Sandeen afirma que estas normas suponen una carga excesiva para las personas que ya están sufriendo.
Diana Barnard, médica de cuidados paliativos de Vermont, aseguró que algunos pacientes ni siquiera pueden ir a sus citas. “Terminan enfermándose más o no quieren viajar, por lo que hay que reprogramar las citas”, explicó. “Se les está pidiendo a los pacientes que utilicen una parte importante de su energía para venir aquí cuando realmente merecen tener la opción más cerca de casa”.
Entre quienes se oponen a la muerte asistida están grupos religiosos que afirman que quitar una vida es inmoral, y médicos que argumentan que su trabajo es hacer que los pacientes terminen sus vidas de manera más confortable, no acabar con la vida en sí.
La antropóloga Anita Hannig, que entrevistó a docenas de enfermos terminales durante la investigación de su libro de 2022, “The Day I Die: The Untold Story of Assisted Dying in America” (“El día que muera: la historia no contada de la muerte asistida en Estados Unidos”), afirmó que no espera que la legislación federal zanje pronto la cuestión. Al igual que hizo con el aborto en 2022, la Corte Suprema en 1997 dictaminó que la muerte asistida era una cuestión de derechos de los estados.
Durante las sesiones legislativas de 2023-24, 19 estados (incluido Pennsylvania, el estado natal de Milano) consideraron la posibilidad de promulgar leyes de muerte asistida, según la organización Compassion & Choices. Delaware fue el único estado que la aprobó, pero el gobernador aún no ha tomado medidas al respecto.
Francine Milano y su esposo, Kris Brackin.(Eric Harkleroad/KFF Health News)
Sandeen señaló que muchos estados aprueban inicialmente leyes restrictivas —que exigen tiempos de espera de 21 días y evaluaciones psiquiátricas, por ejemplo— para acabar derogando las disposiciones que resultan muy complejas. Por eso es optimista y cree que más estados acabarán siguiendo el ejemplo de Vermont y Oregon.
Milano habría preferido viajar a la vecina Nueva Jersey, donde la eutanasia es legal desde 2019, pero su requisito de residencia lo hizo imposible. Y aunque Oregon tiene más proveedores que el estado mayoritariamente rural de Vermont, Milano optó por el viaje en coche de nueve horas a Burlington porque era menos agotador física y financieramente que un viaje a través del país.
La logística era clave porque Milano sabía que tendría que volver. Cuando viajó a Vermont en mayo de 2023 con su marido y su hermano, no estaba al borde de la muerte. Pensó que la próxima vez que fuera a Vermont sería para pedir la medicación. Entonces tendría que esperar 15 días para recibirla.
El período de espera es estándar para garantizar que una persona tenga lo que Barnard llama “un tiempo de reflexión antes de decidirse”, aunque dijo que la mayoría ya lo había hecho mucho antes. Algunos estados han acortado la espera o, como Oregon, pueden solicitar una exención.
Ese tiempo de espera puede ser duro para los pacientes, después de tener que alejarse de su apoyo médico, de su hogar y de su familia. Blanke contó que ha visto hasta 25 familiares asistir a la muerte de un residente de Oregon, pero los que viven fuera del estado suelen traer sólo a una persona.
Y aunque encontrar un lugar donde morir puede ser un problema para los residentes de Oregon que están en residencias o en hospitales que prohíben la muerte asistida, es especialmente difícil para los no residentes.
Cuando Oregon eliminó el requisito de residencia, Blanke publicó un anuncio en Craigslist y utilizó los resultados para recopilar una lista de alojamientos de corto plazo, incluidos Airbnbs, dispuestos a permitir que los pacientes murieran allí. Las organizaciones sin ánimo de lucro en los estados con leyes de muerte asistida también mantienen estas listas, dijo Sandeen.
Milano no ha llegado al punto en que necesite encontrar un lugar donde tomar la medicación y poner fin a su vida. De hecho, como tuvo un año relativamente saludable después de su primer viaje a Vermont, dejó que transcurriera su período de aprobación de seis meses.
En junio, sin embargo, volvió para abrir otro plazo de seis meses. Esta vez fue con una amiga que tiene una casa rodante. Condujeron seis horas para cruzar la frontera del estado, parando en un parque infantil y una tienda de regalos antes de detenerse en un estacionamiento donde Milano tenía una cita de Zoom con sus médicos en lugar de conducir tres horas más hasta Burlington para reunirse en persona.
“No sé si rastrean el GPS o las direcciones de IP, pero me habría dado miedo no ser sincera”, afirmó.
Eso no es lo único que la asusta. Le preocupa estar demasiado enferma para volver a Vermont cuando esté lista para morir. Y, aunque pueda llegar allí, se pregunta si tendrá el valor de tomar la medicación. Alrededor de un tercio de las personas a las que se les aprueba la muerte asistida no lo hacen, explicó Blanke. Para ellos, a menudo es suficiente saber que tienen la medicación —el control— para poner fin a sus vidas cuando lo deseen.
Milano dijo que está agradecida de tener ese poder ahora que aún está lo bastante sana para viajar y disfrutar de la vida. “Ojalá más gente tuviera esa opción”, afirmó.
En junio, Milano fue a Vermont para abrir una segunda ventana de seis meses para recibir ayuda médica para morir. Después de un viaje de seis horas, cruzó la frontera del estado y optó por hablar por Zoom con un médico en lugar de conducir tres horas más para reunirse en persona, como había hecho la primera vez.(Eric Harkleroad/KFF Health News)
Esta historia fue producida por KFF Health News, conocido antes como Kaiser Health News (KHN), una redacción nacional que produce periodismo en profundidad sobre temas de salud y es uno de los principales programas operativos de KFF, la fuente independiente de investigación de políticas de salud, encuestas y periodismo.
In the 18 months after Francine Milano was diagnosed with a recurrence of the ovarian cancer she thought she’d beaten 20 years ago, she traveled twice from her home in Pennsylvania to Vermont. She went not to ski, hike, or leaf-peep, but to arrange to die.
“I really wanted to take control over how I left this world,” said the 61-year-old who lives in Lancaster. “I decided that this was an option for me.”
Dying with medical assistance wasn’t an option when Milano learned in early 2023 that her disease was incurable. At that point, she would have had to travel to Switzerland — or live in the District of Columbia or one of the 10 states where medical aid in dying was legal.
But Vermont lifted its residency requirement in May 2023, followed by Oregon two months later. (Montana effectively allows aid in dying through a 2009 court decision, but that ruling doesn’t spell out rules around residency. And though New York and California recently considered legislation that would allow out-of-staters to secure aid in dying, neither provision passed.)
Despite the limited options and the challenges — such as finding doctors in a new state, figuring out where to die, and traveling when too sick to walk to the next room, let alone climb into a car — dozens have made the trek to the two states that have opened their doors to terminally ill nonresidents seeking aid in dying.
At least 26 people have traveled to Vermont to die, representing nearly 25% of the reported assisted deaths in the state from May 2023 through this June, according to the Vermont Department of Health. In Oregon, 23 out-of-state residents died using medical assistance in 2023, just over 6% of the state total, according to the Oregon Health Authority.
Oncologist Charles Blanke, whose clinic in Portland is devoted to end-of-life care, said he thinks that Oregon’s total is likely an undercount and he expects the numbers to grow. Over the past year, he said, he’s seen two to four out-of-state patients a week — about one-quarter of his practice — and fielded calls from across the U.S., including New York, the Carolinas, Florida, and “tons from Texas.” But just because patients are willing to travel doesn’t mean it’s easy or that they get their desired outcome.
“The law is pretty strict about what has to be done,” Blanke said.
As in other states that allow what some call physician-assisted death or assisted suicide, Oregon and Vermont require patients to be assessed by two doctors. Patients must have less than six months to live, be mentally and cognitively sound, and be physically able to ingest the drugs to end their lives. Charts and records must be reviewed in the state; neglecting to do so constitutes practicing medicine out of state, which violates medical licensing requirements. For the same reason, the patients must be in the state for the initial exam, when they request the drugs, and when they ingest them.
State legislatures impose those restrictions as safeguards — to balance the rights of patients seeking aid in dying with a legislative imperative not to pass laws that are harmful to anyone, said Peg Sandeen, CEO of the group Death With Dignity. Like many aid-in-dying advocates, however, she said such rules create undue burdens for people who are already suffering.
Subscribe to California Healthline’s free Daily Edition.
Diana Barnard, a Vermont palliative care physician, said some patients cannot even come for their appointments. “They end up being sick or not feeling like traveling, so there’s rescheduling involved,” she said. “It’s asking people to use a significant part of their energy to come here when they really deserve to have the option closer to home.”
Those opposed to aid in dying include religious groups that say taking a life is immoral, and medical practitioners who argue their job is to make people more comfortable at the end of life, not to end the life itself.
Anthropologist Anita Hannig, who interviewed dozens of terminally ill patients while researching her 2022 book, “The Day I Die: The Untold Story of Assisted Dying in America,” said she doesn’t expect federal legislation to settle the issue anytime soon. As the Supreme Court did with abortion in 2022, it ruled assisted dying to be a states’ rights issue in 1997.
During the 2023-24 legislative sessions, 19 states (including Milano’s home state of Pennsylvania) considered aid-in-dying legislation, according to the advocacy group Compassion & Choices. Delaware was the sole state to pass it, but the governor has yet to act on it.
Francine Milano with her husband, Kris Brackin.(Eric Harkleroad/KFF Health News)
Sandeen said that many states initially pass restrictive laws — requiring 21-day wait times and psychiatric evaluations, for instance — only to eventually repeal provisions that prove unduly onerous. That makes her optimistic that more states will eventually follow Vermont and Oregon, she said.
Milano would have preferred to travel to neighboring New Jersey, where aid in dying has been legal since 2019, but its residency requirement made that a nonstarter. And though Oregon has more providers than the largely rural state of Vermont, Milano opted for the nine-hour car ride to Burlington because it was less physically and financially draining than a cross-country trip.
The logistics were key because Milano knew she’d have to return. When she traveled to Vermont in May 2023 with her husband and her brother, she wasn’t near death. She figured that the next time she was in Vermont, it would be to request the medication. Then she’d have to wait 15 days to receive it.
The waiting period is standard to ensure that a person has what Barnard calls “thoughtful time to contemplate the decision,” although she said most have done that long before. Some states have shortened the period or, like Oregon, have a waiver option.
That waiting period can be hard on patients, on top of being away from their health care team, home, and family. Blanke said he has seen as many as 25 relatives attend the death of an Oregon resident, but out-of-staters usually bring only one person. And while finding a place to die can be a problem for Oregonians who are in care homes or hospitals that prohibit aid in dying, it’s especially challenging for nonresidents.
When Oregon lifted its residency requirement, Blanke advertised on Craigslist and used the results to compile a list of short-term accommodations, including Airbnbs, willing to allow patients to die there. Nonprofits in states with aid-in-dying laws also maintain such lists, Sandeen said.
Milano hasn’t gotten to the point where she needs to find a place to take the meds and end her life. In fact, because she had a relatively healthy year after her first trip to Vermont, she let her six-month approval period lapse.
In June, though, she headed back to open another six-month window. This time, she went with a girlfriend who has a camper van. They drove six hours to cross the state border, stopping at a playground and gift shop before sitting in a parking lot where Milano had a Zoom appointment with her doctors rather than driving three more hours to Burlington to meet in person.
“I don’t know if they do GPS tracking or IP address kind of stuff, but I would have been afraid not to be honest,” she said.
That’s not all that scares her. She worries she’ll be too sick to return to Vermont when she is ready to die. And, even if she can get there, she wonders whether she’ll have the courage to take the medication. About one-third of people approved for assisted death don’t follow through, Blanke said. For them, it’s often enough to know they have the meds — the control — to end their lives when they want.
Milano said she is grateful she has that power now while she’s still healthy enough to travel and enjoy life. “I just wish more people had the option,” she said.
In June, Milano headed to Vermont to open a second six-month window to receive medical aid in dying. After a six-hour drive, she crossed the state’s border and opted to Zoom with a doctor rather than drive three more hours to meet in person, as she had done the first time.(Eric Harkleroad/KFF Health News)
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
“Vice President Kamala Harris cast the tie-breaking vote to cut, as you know, Medicare by $273 billion. She cast a vote to cut Medicare.”
— Former President Donald Trump at a July 24 campaign rally in Charlotte, North Carolina.
During a July 24 campaign rally in Charlotte, North Carolina, former President Donald Trump claimed that Vice President Kamala Harris was responsible for passing legislation in the U.S. Senate to cut Medicare spending by nearly $300 billion.
“As Vice President, Kamala Harris cast the tie-breaking vote to cut, as you know, Medicare by $273 billion,” Trump told rally attendees. “She cast a vote to cut Medicare.”
Trump gave no further explanation for which vote he was referring to or how he arrived at that figure. A campaign spokesperson told KFF Health News in an email that Trump was referring to a statistic from a Wall Street Journal op-ed by Tomas Philipson, a University of Chicago economist and a former Trump administration official.
Philipson’s op-ed argued that the Inflation Reduction Act — a sweeping climate and health care measure passed in 2022 for which Harris cast the tie-breaking vote — would harm Medicare patients by driving up costs. His article cited a Congressional Budget Office analysis showing that the measure’s health care provisions would reduce the federal deficit by $237 billion over 10 years. “(M)ost of that reduction comes from the program spending less on prescription drugs,” Philipson wrote.
But the government’s spending less on Medicare programs would not amount to the kind of “cut” to Medicare benefits Trump implied, experts told KFF Health News. Several provisions in the law pertaining to prescription drug pricing are widely seen by health policy experts as beneficial to both consumers and the government. Individual patients are expected to spend less out-of-pocket on their prescription drugs, while the government will reduce Medicare spending without any impact to services offered.
We dug into the facts surrounding Trump’s claim and the law’s effect on Medicare. It resurfaces a long-running debate over Medicare savings versus cuts and the question of whether lowered spending automatically leads to a reduction in benefits for Medicare enrollees.
Subscribe to California Healthline’s free Daily Edition.
Following the Numbers
The Inflation Reduction Act’s many provisions include some intended to lower prescription drug costs for older Americans and others receiving Medicare insurance coverage.
The law caps the cost of insulin at $35 per month for most Medicare beneficiaries, establishes out-of-pocket spending limits for Part D drug coverage, and institutes penalties for drug companies that raise prices faster than the inflation rate. The law also authorizes Medicare officials, for the first time, to negotiate drug pricing directly with pharmaceutical manufacturers.
“The idea behind drug price negotiation is that Medicare can use its buying power to get a better price than what is currently being negotiated for these drugs,” said Juliette Cubanski, deputy director of the program on Medicare policy at KFF, a health information nonprofit that includes KFF Health News.
According to an analysis by the Congressional Budget Office, the nonpartisan federal agency that calculates the financial impact of new legislation, the Inflation Reduction Act’s health care measures will have a mixed effect on spending. Some steps, such as the cap on beneficiaries’ out-of-pocket prescription drug spending, will likely cost the government more. But others, including the drug price negotiations, are projected to save the government money. All told, the Inflation Reduction Act’s health care measures are expected to save taxpayers $237 billion over 10 years.
On the numbers, Trump said the law would “cut Medicare” by $273 billion; he likely meant $237 billion.
Despite the government being expected to spend less overall, beneficiaries’ services would not necessarily be cut, as Trump claimed. In fact, most Medicare recipients would likely see their costs decrease, too, while keeping the same level of benefits.
“There are big shifts in who’s paying for what,” said Andrew Mulcahy, a senior health economist who researches prescription drug markets at the Rand Corp., a nonpartisan think tank. “But that doesn’t mean they’re getting any less. If anything, they’ll have better access to drugs.”
Cubanski, echoing Mulcahy, said: “When you’re reducing Medicare spending, that’s not the same thing as a cut to Medicare or cutting Medicare benefits. If you buy eggs every week and now you’re getting them cheaper, you’re still getting the eggs, you’re just getting them for a lower price.”
A year ago, the Centers for Medicare & Medicaid Services named the first 10 drugs on which it will focus, though the exact savings from the drug pricing negotiations process will be known only when the government and drug manufacturers reach agreements. The new pricing for this first batch of medications is set to take effect in 2026.
Whether the government can negotiate meaningfully lower costs versus current prices is unclear, especially since pharmacy benefit managers, or PBMs — middlemen in the negotiations among drug companies, insurers and pharmacies — are tasked with doing that.
“I think for many of the drugs selected in the first year, my expectation is that the government won’t be able to do much better than the PBMs,” Mulcahy told KFF Health News.
The Medicare drug pricing program could have negative side effects. Philipson, for example, argued in his op-ed that the negotiations will “deter companies from developing new medicines” and threaten older Americans’ access to doctors, as manufacturers and hospitals would likely be reimbursed less for their drugs and services.
Cubanski brushed off such concerns.
“The drug industry certainly has a vested interest, you know, in raising alarm bells,” she said. “I think it’s just still too early to talk about ‘the sky is falling’ with regard to pharmaceutical innovation. Time will tell, but it certainly is the case right now that the law includes a lot of provisions that will be very helpful for Medicare beneficiaries.”
On Aug. 15, CMS announced the results of its negotiation over the first round of drugs. The new prices represent discounts ranging from 38% to 79% of the original costs. White House officials said the negotiations will lead to $6 billion in savings for Medicare the first year, while Medicare recipients are expected to save an additional $1.5 billion in out-of-pocket costs.
Our Ruling
Trump’s statement is wrong both on the hard numbers and his interpretation of what they mean.
The analysis Trump cited, per his campaign, said the Inflation Reduction Act’s health care provisions would lower the deficit by $237 billion — not $273 billion, as the former president claimed. Moreover, whatever the exact number is, multiple experts pushed back against the notion that the savings equated to a “cut” to Medicare, as Trump claimed.
Phone interview with Andrew Mulcahy, senior health economist at Rand Corp., July 26, 2024.
Phone interview with Juliette Cubanski, deputy director of the program on Medicare policy at KFF, July 29, 2024.
United States Senate, Roll Call Vote 117th Congress-2nd Session, Aug. 7, 2022.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
Newswise — University of Maryland School of Medicine (UMSOM) Dean Mark T. Gladwin, MD, announced today the appointment of Kelly Dunn, PhD, MBA, one of the nation’s leading researchers on opioid use disorder, as the inaugural Director of the School’s Kahlert Institute for Addiction Medicine. She will also serve as a Professor in the Department of Psychiatry with a secondary appointment in the Department of Neurobiology at UMSOM.
Dr. Dunn is currently a Professor of Psychiatry and Behavioral Sciences at Johns Hopkins School of Medicine with a joint appointment in Health Policy and Management at the Johns Hopkins University School of Public Health.
Dr. Dunn has been the Principal Investigator on projects totaling more than $21 million in awards from the National Institutes of Health. She has authored more than 130 peer-reviewed publications in the area of substance use and opioid use disorder.
The Kahlert Institute for Addiction Medicine, launched in 2023 with a major gift from the Kahlert Foundation, is uniquely positioned to bring together leading addiction experts from across basic science and clinical care to transform the prevention, treatment, education, and research of addiction.
“With addiction, substance use disorder, and overdose deaths reaching epidemic proportions here in Maryland and in the U.S., we are extremely pleased to attract a top academician and leader in this field to move the Institute forward with a long-term impact,” said Dean Gladwin.
Growing up in rural Central New York in the late 1990’s, Dr. Dunn watched several close friends become dependent on opioids, after first being exposed through prescription medications, and eventually go on to develop opioid use disorder (OUD). “This prompted my life-long passion for understanding motivations for opioid use, identifying methods to prevent the onset of OUD, and helping to improve treatments for OUD,” said Dr. Dunn. “I’m honored and thrilled to take the helm of the Kahlert Institute and to work together with all of the stellar faculty who are world-class leaders in addiction research to advance the science of addiction medicine.”
Since 2012, Dr. Dunn has been a faculty member in the Johns Hopkins University Behavioral Pharmacology Research Unit (BPRU) located within the Department of Psychiatry and Behavioral Sciences. Her current work focuses on the conduct of Phase II/III randomized controlled assessments of medications, mainly those targeted for opioid use disorder.
She has also managed trials focused on treatments for cigarette smoking and alcohol use disorder and has conducted several basic science human laboratory examinations of drug effects, which is complemented by a body of work focused on epidemiological and machine-learning analyses of publicly available datasets.
She has held multiple leadership roles in the substance use field, including serving as President for the American Psychological Association’s Society for Psychopharmacology and Substance Use and the College on the Problems of Drug Dependence (CPDD) as well as Co-Editor of the Journal of Addiction Medicine and Editor-in-Chief of the journal Experimental and Clinical Psychopharmacology.
“Dr. Dunn’s current work in the field is impressive,”saidGreg Kahlert,President of The Kahlert Foundation. “I am confident with her experience, passion and collaborative spirit, she will help find treatments and cures for those suffering from addiction. I could not be more excited that she is the first director of the Kahlert Institute for Addiction Medicine.”
Dr. Dunn is currently the principal investigator on a multisite examination of a treatment for co-morbid pain in people with opioid use disorder. She is also an investigator on a Phase II trial examining the use of the drug suvorexant to treat sleep disorders, withdrawal, and craving in people initiating treatment with buprenorphine for opioid use disorder.
Other studies include a combination laboratory/clinical trial examining phenotypes of opioid withdrawal and a pilot trial examination of suvorexant for cocaine use in people being treated for OUD. Dr. Dunn recently completed a series of human laboratory trials examining genetic contributions to opioid sensitivity and opioid-cannabinoid interactions for pain treatment in healthy and clinical populations.
In addition to her numerous peer-reviewed original and review publications, Dr. Dunn edited the Oxford Handbook on Opioids and Opioid Use Disorder. She received her PhD Degree from the University of Vermont in 2009 and earned an MBA Degree from Johns Hopkins University Carey School of Business in 2019.