In 1942, a young Black man named Cleo Wright was removed from a Sikeston, Missouri, jail and lynched by a white mob.
Nearly 80 years later, another young Black man, Denzel Taylor, was shot at least 18 times by police in the same small community.
In the hourlong “Silence in Sikeston” documentary film broadcast on WORLD’s “Local, USA,” KFF Health News and Retro Report explore how the impact of these men’s killings tells a story about trauma and racism, but also resilience and healing.
Stemming from a reporting trip by KFF Health News Midwest correspondent Cara Anthony in 2020, this film takes the audience to Indiana, Alabama, and where it all began in the southeastern corner of Missouri known as the Bootheel.
Wright’s lynching put this rural community on a world stage and led to the first federal attempt to prosecute a lynching. But no one was held accountable. The killing was quickly hushed among locals, and his name was largely forgotten. When Taylor was shot by police in 2020 —a year when protests about police brutality rocked the nation — his killing drew little attention.
The film breaks the silence and shares the stories of these men’s families, community members, and police to uncover the consequences of this trauma on Sikeston. A limited-series podcast exploring the health effects of racial violence and articles are also part of this journalism collaboration.
“Being quiet isn’t the answer,” Michael Snider, Cleo Wright’s great-grandson, told the filmmakers.
Credits
KFF Health News
Producer and reporter: Cara Anthony Editors: Taunya English, Kytja Weir Copy editors: Terry Byrne, Gabe Brison-Trezise Web producers: Lynne Shallcross, Oona Zenda, Lydia Zuraw Photographer: Michael B. Thomas Social media producers: Tarena Lofton, Hannah Norman
Retro Report
Director: Jill Rosenbaum Writer: Jill Rosenbaum Editors: Cheree Dillon, Brian Kamerzel Senior producer: Karen M. Sughrue Executive producer: Kyra Darnton
WORLD
Host: Tina M. McDuffie Producer and editor: Hannah Paul Digital producer: Sharon Wong Editor: Jill Poisson, Cecilia Préstamo Assistant editor: Abhi Indrekar Digital associate producer: Brigitte McIndoe Post-production assistant: Jenny Tan Senior editorial adviser: Judith Vecchione Project manager, acquisition and distribution: Georgiana Lee
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
Gerri Norington, 78, never wanted to be on her own as she grew old.
But her first marriage ended in divorce, and her second husband died more than 30 years ago. When a five-year relationship came to a close in 2006, she found herself alone — a situation that has lasted since.
“I miss having a companion who I can talk to and ask ‘How was your day?’ or ‘What do you think of what’s going on in the world?’” said Norington, who lives in an apartment building for seniors on the South Side of Chicago. Although she has a loving daughter in the city, “I don’t want to be a burden to her,” she said.
Norington is part of a large but often overlooked group: the more than 16 million Americans living alone while growing old. Surprisingly little is known about their experiences.
This slice of the older population has significant health issues: Nearly 4 in 10 seniors living alone have vision or hearing loss, difficulty caring for themselves and living independently, problems with cognition, or other disabilities, according to a KFF analysis of 2022 census data.
If help at home isn’t available when needed — an altogether too common problem — being alone can magnify these difficulties and contribute to worsening health.
Multiple studies find that seniors on their own are at higher risk of becoming isolated, depressed, and inactive, having accidents, and neglecting to care for themselves. As a result, they tend to be hospitalized more often and suffer earlier-than-expected deaths.
Getting medical services can be a problem, especially if older adults living alone don’t drive or live in rural areas. Too often, experts observe, health care providers don’t ask about older adults’ living situations and are unaware of the challenges they face.
***
During the past six months, I’ve spoken to dozens of older adults who live alone either by choice or by circumstance — most commonly, a spouse’s death. Some have adult children or other close relatives who are involved in their lives; many don’t.
In lengthy conversations, these seniors expressed several common concerns: How did I end up alone at this time of life? Am I OK with that? Who can I call on for help? Who can make decisions on my behalf if I’m unable to? How long will I be able to take care of myself, and what will happen when I can’t?
This “gray revolution” in Americans’ living arrangements is fueled by longer life spans, rising rates of divorce and childlessness, smaller families, the geographic dispersion of family members, an emphasis on aging in place, and a preference for what Eric Klinenberg, a professor of sociology at New York University, calls “intimacy at a distance” — being close to family, but not too close.
Subscribe to California Healthline’s free Daily Edition.
The most reliable, up-to-date data about older adults who live alone comes from the U.S. Census Bureau. According to its 2023 Current Population Survey, about 28% of people 65 and older live by themselves, including slightly fewer than 6 million men and slightly more than 10 million women. (The figure doesn’t include seniors living in institutions, primarily assisted living and nursing homes.)
By contrast, 1 in 10 older Americans lived on their own in 1950.
Ken Elliott, a retired psychology professor, lives by himself in a house in Mount Vernon, Maine. His only living relative is a brother in California. Elliott is thinking about how to put together a team of people who can help him age in place. “Aging without a mythic family support system — which everyone assumes people have — is tough for everybody,” Elliott says. (Ken Elliott)
“I like being alone better than I like being in relationships,” says Janice Chavez of Denver. “I don’t have to ask anybody for anything. If I want to sleep late, I sleep late. If I want to stay up and watch TV, I can. I do whatever I want to do. I love the independence and the freedom.” (Judith Graham for KFF Health News)
This is, first and foremost, an older women’s issue, because women outlive men and because they’re less likely to remarry after being widowed or divorcing. Twenty-seven percent of women ages 65 to 74 live alone, compared with 21% of men. After age 75, an astonishing 43% of women live alone, compared with only 24% for men.
The vast majority — 80% — of people who live alone after age 65 are divorced or widowed, twice the rate of the general population, according to KFF’s analysis of 2022 census data. More than 20% have incomes below $13,590, the federal poverty line in 2022, while 27% make between that and $27,180, twice the poverty level.
***
Of course, their experiences vary considerably. How older adults living alone are faring depends on their financial status, their housing, their networks of friends and family members, and resources in the communities where they live.
Attitudes can make a difference. Many older adults relish being independent, while others feel abandoned. It’s common for loneliness to come and go, even among people who have caring friends and family members.
“I like being alone better than I like being in relationships,” said Janice Chavez of Denver, who said she’s in her 70s. “I don’t have to ask anybody for anything. If I want to sleep late, I sleep late. If I want to stay up and watch TV, I can. I do whatever I want to do. I love the independence and the freedom.”
Chavez is twice divorced and has been on her own since 1985. As a girl, she wanted to be married and have lots of kids, but “I picked jerks,” she said. She talks to her daughter, Tracy, every day, and is close to several neighbors. She lives in the home she grew up in, inherited from her mother in 1991. Her only sibling, a brother, died a dozen years ago.
In Chicago, Norington is wondering whether to stay in her senior building or move to the suburbs after her car was vandalized this year. “Since the pandemic, fear has almost paralyzed me from getting out as much as I would like,” she told me.
She’s a take-charge person who has been deeply involved in her community. In 2016, Norington started an organization for single Black seniors in Chicago that sponsored speed dating events and monthly socials for several years. She volunteered with a local medical center doing outreach to seniors and brought health and wellness classes to her building. She organized cruises for friends and acquaintances to the Caribbean and Hawaii in 2022 and 2023.
Now, every morning, Norington sends a spiritual text message to 40 people, who often respond with messages of their own. “It helps me to feel less alone, to feel a sense of inclusion,” she said.
Lester Shane lives alone in an 11-by-14 studio apartment in New York City. “There are days when I’m carrying my groceries up three flights of stairs when I think, ‘This is really hard,’” Shane says. (Judith Graham for KFF Health News)
In Maine, Ken Elliott, 77, a retired psychology professor, lives by himself in a house in Mount Vernon, a town of 1,700 people 20 miles northwest of the state capital. He never married and doesn’t have children. His only living relative is an 80-year-old brother in California.
For several years, Elliott has tried to raise the profile of solo agers among Maine policymakers and senior organizations. This began when Elliott started inquiring about resources available to older adults living by themselves, like him. How were they getting to doctor appointments? Who was helping when they came home from the hospital and needed assistance? What if they needed extra help in the home but couldn’t afford it?
To Elliott’s surprise, he found this group wasn’t on anyone’s radar, and he began advocating on solo agers’ behalf.
Now, Elliott is thinking about how to put together a team of people who can help him as he ages in place — and how to build a stronger sense of community. “Aging without a mythic family support system — which everyone assumes people have — is tough for everybody,” Elliott said.
In Manhattan, Lester Shane, 72, who never married or had children, lives by himself in an 11-by-14-foot studio apartment on the third floor of a building without an elevator. He didn’t make much money during a long career as an actor, a writer, and a theater director, and he’s not sure how he’ll make ends meet once he stops teaching at Pace University.
“There are days when I’m carrying my groceries up three flights of stairs when I think, ‘This is really hard,’” Shane told me. Although his health is pretty good, he knows that won’t last forever.
“I’m on all the lists for senior housing — all lottery situations. Most of the people I’ve talked to said you will probably die before your number comes up,” he said with mordant humor.
Then, Shane turned serious. “I’m old and getting older, and whatever problems I have now are only going to get worse,” he said. As is the case for many older adults who live alone, his friends are getting older and having difficulties of their own.
The prospect of having no one he knows well to turn to is alarming, Shane admitted: “Underneath that is fear.”
Kate Shulamit Fagan, 80, has lived on her own since 1979, after two divorces. “It was never my intention to live alone,” she told me in a lengthy phone conversation. “I expected that I would meet someone and start another relationship and somehow sail off into the rest of my life. It’s been exceedingly hard to give up that expectation.”
When I first spoke to Fagan, in mid-March, she was having difficulty in Philadelphia, where she’d moved two years earlier to be close to one of her sons. “I’ve been really lonely recently,” she told me, describing how difficult it was to adjust to a new life in a new place. Although her son was attentive, Fagan desperately missed the close circle of friends she’d left behind in St. Petersburg, Florida, where she’d lived and worked for 30 years.
Four and a half months later, when I called Fagan again, she’d returned to St. Petersburg and was renting a one-bedroom apartment in a senior building in the center of the city. She’d celebrated her birthday there with 10 close friends and was meeting people in her building. “I’m not completely settled, but I feel fabulous,” she told me.
What accounted for the change? “Here, I know if I want to go out or I need help, quite a few people would be there for me,” Fagan said. “The fear is gone.”
As I explore the lives of older adults living alone in the next several months, I’m eager to hear from people who are in this situation. If you’d like to share your stories, please send them to [email protected].
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
A seemingly innocuous proposal to offer scholarships for mental health workers in California’s new court-ordered treatment program has sparked debate over whether the state should prioritize that program or tackle a wider labor shortage in behavioral health services.
Nine counties have begun rolling out the Community Assistance, Recovery, and Empowerment Act, which Gov. Gavin Newsom (D) signed into law in 2022 to get people with untreated schizophrenia or other psychotic disorders, many of them incarcerated or homeless, into treatment. But often those skilled clinicians have been pulled by counties from other understaffed behavioral health programs.
“There’s just so much change coming with a limited workforce, limited treatment resources, and high expectations for counties to solve things like homelessness,” said Scott Kennelly, director of the Butte County Behavioral Health Department. “It’s like I’m turning on a fire hose and saying, ‘Start drinking.’”
The bill by state Sen. Tom Umberg would create an annual scholarship fund for students who pursue a mental health profession provided they work for three years with CARE Court. Umberg had requested $10 million for the program, but it’s unclear how many students would receive the scholarship, said Jackie Koenig, a spokesperson for the senator. The bill sailed through the legislature without a single lawmaker voting against it.
Umberg, a Democrat from Santa Ana, said CARE Court deserves targeted funding because it’s a new program, and he noted other state scholarships are available for students pursuing a behavioral health degree. For instance, the state announced in March 2023 that it would issue $118 million in grants to support behavioral health providers at 134 nonprofit community-based organizations.
“CARE Court is new, and it is in a unique space that requires unique behavioral health skills, dealing with schizophrenics,” Umberg said. “So, we want to encourage folks to go into that space, because it is a challenge.”
Subscribe to California Healthline’s free Daily Edition.
But local behavioral health administrators say shifting experts into CARE Court may create shortages in other programs or thrust mental health specialists into multiple demanding programs.
The CARE Act allows patients or others, such as their relatives, behavioral health care providers, or roommates, to petition their county court for help. Individuals who agree to participate can receive up to 24 months of treatment, which can include outpatient substance use disorder treatment, stabilization medication, connection to social services, and housing. It is one of Newsom’s experimental initiatives intended to get some of the state’s 181,000 homeless people off the streets and into housing without resorting to mandatory conservatorships.
Only 7,000 to 12,000 Californians are estimated to be eligible for treatment, according to the Judicial Council, which helps oversee the program.
The state has allocated $251 million to staff and launch the CARE program through the current budget year, including $122 million in grants to counties, according to the state Legislative Analyst’s Office. At the same time, counties have been directed to implement a host of other behavioral health programs, such as mobile crisis teams, and boost mental health services for Medi-Cal patients. Last year, Newsom also signed legislation that broadened the number of Californians who could be involuntarily committed.
“As a high-profile mandate, counties are largely moving existing, skilled, experienced staff over to launch and staff the CARE Court teams,” said Michelle Cabrera, executive director of the County Behavioral Health Directors Association of California, which supports the bill.
It’s why critics, including ACLU California Action, Mental Health America of California, and some counties, say a CARE Court scholarship should also support other county programs that treat individuals with serious mental illness and housing instability.
“Restricting workforce development initiatives solely to one of the many new behavioral health initiatives will not solve the issues of staffing across the continuum of behavioral health services,” said Alexandra Pierce, an assistant director at the Merced County Behavioral Health and Recovery Services Department.
County behavioral health departments are in the midst of a massive behavioral health workforce shortage — running 25% to 30% below full staff capacity, on average, according to an internal 2023 survey conducted by the county behavioral health director association and the University of California-San Francisco’s Healthforce Center, Cabrera said.
More than a dozen rural and urban county behavioral health directors told California Healthline that hiring challenges are widespread and not unique to CARE Court, pointing to burnout since the start of the covid-19 pandemic and steep competition from schools, correctional facilities, and the private sector, which can offer skilled clinicians higher pay, work-from-home telehealth jobs, and generous vacation.
Michelle Funez, division director of Marin County Behavioral Health and Recovery Services, said a CARE Court scholarship could incentivize students to pursue county jobs that support vulnerable individuals in the community.
Finding the right clinician for CARE Court can be tricky because the job requires skilled individuals to work in homeless encampments and other nontraditional environments, Funez said.
“It can feel like we’re looking for the needle in the haystack,” Funez said, drawing from “an already smaller body of staff who have the requisite skills for this type of work, who are also up for the challenge.”
The nine counties that have launched the specialized courts have received more than 600 petitions in the first 10 months of the program, said Leah Myers, a spokesperson for the state Department of Health Care Services, which helps oversee the program. The remaining 49 counties are slated to launch their programs by Dec. 1.
There have been early successes with the program. A year in, San Diego County is already beginning to “graduate” patients, meaning they have received treatment and have made enough progress to transition out of the court system.
As more counties roll out CARE Courts, they will need more clinicians. A scholarship program, some counties said, could help. But the bill’s price tag could be its downfall. In June, Newsom signed a state budget closing an estimated $46.8 billion deficit, and last year he vetoed hundreds of bills, many of them over cost. Newsom spokesperson Elana Ross declined to comment on the measure.
Newsom has until the end of the month to sign or veto the bill.
SACRAMENTO — California Gov. Gavin Newsom will soon decide whether the most populous U.S. state will join 25 others in regulating the middlemen known as pharmacy benefit managers, or PBMs, whom many policymakers blame for the soaring cost of prescription drugs.
PBMs have been under fire for years for alleged profiteering and anticompetitive conduct, but efforts to regulate the industry at the federal level have stalled in Congress.
The three largest PBMs are owned by insurers and retail pharmacy chains, and about 80% of prescription drug sales in the United States are controlled by them: OptumRx, owned by UnitedHealth Group; CVS Caremark, owned by CVS Health, which also owns the insurer Aetna; and Express Scripts, owned by The Cigna Group.
The proposed law, spearheaded by state Sen. Scott Wiener of San Francisco, a Democrat, would require PBMs to apply for a license by 2027 and would mandate that licensed PBMs pass along 100% of pharmaceutical manufacturers’ rebates to health plans or insurers. Drug companies often offer substantial discounts on medications to boost demand, and one of the major criticisms of PBMs is that they pocket rebates rather than pass savings along to customers.
The law would also mostly bar PBMs from steering patients to pharmacies they own, which includes the major mail-order pharmacies. And it would prohibit them from giving independent pharmacies lower insurance reimbursements than they offer the big chains — a major issue for the dwindling number of independents around the country.
Wiener said the law aimed to rein in what he called “the worst abuses by PBMs.” Proponents of the legislation say the experiences in the 25 states that require PBM licensing and the 16 that ban steering of patients to preferred vendors show that regulations reduce costs for consumers.
“When they’re licensed like we’re looking at, the cost goes down. States without licensing saw costs go up,” said Assembly member Devon Mathis, one of two Republicans to co-author the bill, citing the National Community Pharmacists Association.
Subscribe to California Healthline’s free Daily Edition.
Health insurance premiums increased an average of 16.7% nationwide from 2015 to 2019, the association calculated, with premiums in states that license PBMs increasing 0.3 of a percentage point below the national average and those without, 0.4 above. The association claimed similar benefits from several other reforms affecting pharmacies.
The Pharmaceutical Care Management Association, which represents pharmacy benefit managers, said Wiener’s bill “blatantly” favors independent retail pharmacies over chains.
“This legislation does nothing to lower costs for patients; it simply seeks to financially promote one industry over another with no consumer benefit,” the group said.
Insurance companies argue that the California bill would reduce the PBMs’ ability to negotiate lower drug prices, resulting in higher coverage premiums for everyone. But drugmakers argue that reforms don’t raise premiums.
Supreme Court Decision Looms
States have stepped in to regulate PBMs in the absence of any federal action; Congress has been holding oversight hearings on PBMs, and the Federal Trade Commission in July said PBMs “may be profiting by inflating drug costs and squeezing Main Street pharmacies,” but there has been no new legislation or efforts to crack down based on existing laws barring anticompetitive conduct.
The U.S. Supreme Court could soon weigh in on whether states have the authority to regulate PBMs. A federal appellate court blocked Oklahoma regulations on PBMs on the grounds that federal law held sway, and a group of 35 state attorneys general, including California’s Rob Bonta, have asked the Supreme Court to overturn the ruling.
A central complaint about PBMs is that they take money from pharmaceutical companies, in the form of “rebates,” to give their drugs preferential treatment on health plans’ lists of medications that are covered by insurance, known as formularies. Those rebates may play a role in raising drug prices, found a 2020 paper by the University of Southern California’s Schaeffer Center for Health Policy & Economics.
Under the California bill, those rebates are to be used “for the sole purpose of lowering deductibles and out-of-pocket cost for consumers,” said Assembly member Jim Wood, a Democrat. “There is a perverse incentive by PBMs to choose for their formulary the drugs that will give them the biggest rebate, the largest rebate, even if there are other drugs just as effective and lower-cost. That alone should send shivers down your spine.”
Crackdown in California
California collected more than $215 million last year from the nation’s largest Medicaid insurer, Centene, after it failed to disclose or pass along drug discounts negotiated by its PBM to the state Medicaid agency.
Independent pharmacies say provisions in the proposed California law requiring PBMs to offer them the same pricing as the chains could be a lifeline.
Clint Hopkins, who has co-owned Pucci’s Pharmacy in Sacramento for eight years, said he’s forced to regularly turn away customers rather than lose hundreds of dollars each time he fills their high-cost prescriptions.
For instance, he said his cost for a monthly dose of Biktarvy, used to treat HIV, is $3,881.68. But he said pharmacy benefit managers short him up to $360 on the reimbursement.
“They dictate the rates to us, and they will not negotiate,” said Hopkins, who testified for the bill on behalf of the California Pharmacists Association. “Sometimes I have to say, ‘I’m sorry, I want to help you, but I can’t lose this much money on your prescription.’”
While the bill passed with unusual legislative support, it faces an uncertain future with the Democratic governor, who has until Sept. 30 to sign or veto it.
Newsom vetoed a 2021 bill that would have barred PBMs from steering patients to their own pharmacies, citing potential unintended consequences.
And his Department of Finance said administering the licensing and collecting the data required by the law would cost several million dollars. In vetoing other legislation, Newsom has repeatedly cited costs, as the state struggles with a massive budget deficit.
If you or someone you know may be experiencing a mental health crisis, contact the 988 Suicide & Crisis Lifeline by dialing or texting “988.”
When Pooja Mehta’s younger brother, Raj, died by suicide at 19 in March 2020, she felt “blindsided.”
Raj’s last text message was to his college lab partner about how to divide homework questions.
“You don’t say you’re going to take questions 1 through 15 if you’re planning to be dead one hour later,” said Mehta, 29, a mental health and suicide prevention advocate in Arlington, Virginia. She had been trained in Mental Health First Aid — a nationwide program that teaches how to identify, understand, and respond to signs of mental illness — yet she said her brother showed no signs of trouble.
Mehta said some people blamed her for Raj’s death because the two were living together during the covid-19 pandemic while Raj was attending classes online. Others said her training should have helped her recognize he was struggling.
But, Mehta said, “we act like we know everything there is to know about suicide prevention. We’ve done a really good job at developing solutions for a part of the problem, but we really don’t know enough.”
Raj’s death came in the midst of decades of unsuccessful attempts to tamp down suicide rates nationwide.
Pooja Mehta, a mental health advocate, with her younger brother, Raj, who died by suicide in March 2020. Raj’s death came in the midst of decades of unsuccessful attempts to lower suicide rates nationwide. “We’ve done a really good job at developing solutions for a part of the problem,” Mehta says. “But we really don’t know enough.”(Portia Eastman)
During the past two decades federal officials have launched three national suicide prevention strategies, including one announced in April.
The first strategy, announced in 2001, focused on addressing risk factors for suicide and leaned on a few common interventions.
The next strategy called for developing and implementing standardized protocols to identify and treat people at risk for suicide with follow-up care and the support needed to continue treatment.
The latest strategy builds on previous ones and includes a federal action plan calling for implementation of 200 measures over the next three years, including prioritizing populations disproportionately affected by suicide, such as Black youth and Native Americans and Alaska Natives.
Subscribe to California Healthline’s free Daily Edition.
Despite those evolving strategies, from 2001 through 2021 suicide rates increased most years, according to the Centers for Disease Control and Prevention. Provisional data for 2022, the most recent numbers available, shows deaths by suicide grew an additional 3% over the previous year. CDC officials project the final number of suicides in 2022 will be higher.
In the past two decades, suicide rates in rural states such as Alaska, Montana, North Dakota, and Wyoming have been about double those in urban areas, according to the CDC.
Despite those persistently disappointing numbers, mental health experts contend the national strategies aren’t the problem. Instead, they argue, the policies — for many reasons —simply aren’t being funded, adopted, and used. That slow uptake was compounded by the covid-19 pandemic, which had a broad, negative impact on mental health.
A chorus of national experts and government officials agree the strategies simply haven’t been embraced widely, but said even basic tracking of deaths by suicide isn’t universal.
Surveillance data is commonly used to drive health care quality improvement and has been helpful in addressing cancer and heart disease. Yet, it hasn’t been used in the study of behavioral health issues such as suicide, said Michael Schoenbaum, a senior adviser for mental health services, epidemiology, and economics at the National Institute of Mental Health.
“We think about treating behavioral health problems just differently than we think about physical health problems,” Schoenbaum said.
Without accurate statistics, researchers can’t figure out who dies most often by suicide, what prevention strategies are working, and where prevention money is needed most.
Many states and territories don’t allow medical records to be linked to death certificates, Schoenbaum said, but NIMH is collaborating with a handful of other organizations to document this data for the first time in a public report and database due out by the end of the year.
Further hobbling the strategies is the fact that federal and local funding ebbs and flows and some suicide prevention efforts don’t work in some states and localities because of the challenging geography, said Jane Pearson, special adviser on suicide research to the NIMH director.
Wyoming, where a few hundred thousand residents are spread across sprawling, rugged landscape, consistently ranks among the states with the highest suicide rates.
State officials have worked for many years to address the state’s suicide problem, said Kim Deti, a spokesperson for the Wyoming Department of Health.
But deploying services, like mobile crisis units, a core element of the latest national strategy, is difficult in a big, sparsely populated state.
“The work is not stopping but some strategies that make sense in some geographic areas of the country may not make sense for a state with our characteristics,” she said.
Lack of implementation isn’t only a state and local government problem. Despite evidence that screening patients for suicidal thoughts during medical visits helps head off catastrophe, health professionals are not mandated to do so.
Many doctors find suicide screening daunting because they have limited time and insufficient training and because they aren’t comfortable discussing suicide, said Janet Lee, an adolescent medicine specialist and associate professor of pediatrics at the Lewis Katz School of Medicine at Temple University.
“I think it is really scary and kind of astounding to think if something is a matter of life and death how somebody can’t ask about it,” she said.
The use of other measures has also been inconsistent. Crisis intervention services are core to the national strategies, yet many states haven’t built standardized systems.
Besides being fragmented, crisis systems, such as mobile crisis units, can vary from state to state and county to county. Some mobile crisis units use telehealth, some operate 24 hours a day and others 9 to 5, and some use local law enforcement for responses instead of mental health workers.
Only 23% of Americans are familiar with 988 and there’s a significant knowledge gap about the situations people should call 988 for, according to a recent poll conducted by the National Alliance on Mental Illness and Ipsos.
A bookmark for children with the 988 Suicide & Crisis Lifeline number is displayed by Lance Neiberger, a volunteer with the Natrona County Suicide Prevention Task Force, in Casper, Wyoming, on Aug. 14, 2022.(Patrick T. Fallon/AFP via Getty Images)
Most states, territories, and tribes have also not yet permanently funded 988, which was launched nationwide in July 2022 and has received about $1.5 billion in federal funding, according to the Substance Abuse and Mental Health Services Administration.
Anita Everett, director of the Center for Mental Health Services within SAMHSA, said her agency is running an awareness campaign to promote the system.
Some states, including Colorado, are taking other steps. There, state officials installed financial incentives for implementing suicide prevention efforts, among other patient safety measures, through the state’s Hospital Quality Incentive Payment Program. The program hands out about $150 million a year to hospitals for good performance. In the last year, 66 hospitals improved their care for patients experiencing suicidality, according to Lena Heilmann, director of the Office of Suicide Prevention at the Colorado Department of Public Health and Environment.
Experts hope other states will follow Colorado’s lead.
And despite the slow movement, Mehta sees bright spots in the latest strategy and action plan.
Although it is too late to save Raj, “addressing the social drivers of mental health and suicide and investing in spaces for people to go to get help well before a crisis gives me hope,” Mehta said.
Cheryl Platzman Weinstock’s reporting is supported by a grant from the National Institute for Health Care Management Foundation.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
Si tú o alguien que conoces pudiera estar pasando por una crisis de salud mental, comunícate con la línea directa de suicidio y crisis 988, marcando o enviando un mensaje de texto al “988”.
Cuando el hermano menor de Pooja Mehta, Raj, murió por suicidio a los 19 años en marzo de 2020, ella se sintió “inesperadamente sorprendida”.
El último mensaje de texto de Raj fue para su compañero de laboratorio en la universidad sobre cómo organizar las preguntas de una tarea.
“No dices que vas a tomar las preguntas del 1 al 15 si planeas estar muerto una hora después”, dijo Mehta, de 29 años, defensora de salud mental y prevención del suicidio en Arlington, Virginia. Había recibido capacitación en Primeros Auxilios de Salud Mental, un programa nacional que enseña cómo identificar, comprender y responder a las señales de enfermedad mental. Sin embargo, dijo que su hermano no mostró signos de problemas.
Mehta dijo que algunas personas la culparon por la muerte de Raj porque los dos vivían juntos durante la pandemia de covid-19, mientras Raj tomaba clases por internet. Otros dijeron que su capacitación debería haberla ayudado a reconocer que su hermano estaba en crisis.
Pero Mehta dijo que “actuamos como si supiéramos todo lo que hay que saber sobre la prevención del suicidio. Hemos hecho un buen trabajo desarrollando soluciones para parte del problema, pero realmente no sabemos lo suficiente”.
La muerte de Raj ocurrió en medio de décadas de intentos fallidos para reducir las tasas de suicidio a nivel nacional.
Durante los últimos 20 años, funcionarios federales han lanzado tres estrategias nacionales de prevención del suicidio, incluida una anunciada en abril.
La primera estrategia, de 2001, se centró en abordar los factores de riesgo del suicidio y se basó en algunas intervenciones comunes.
La siguiente, pidió desarrollar e implementar protocolos estandarizados para identificar y tratar a personas en riesgo de suicidio, con seguimiento y el apoyo necesario para continuar el tratamiento.
La iniciativa más reciente se basa en las anteriores e incluye un plan de acción federal que llama a implementar 200 medidas durante los próximos tres años, incluidas priorizar a las poblaciones desproporcionadamente afectadas por el suicidio, como los jóvenes negros, los nativos americanos y de Alaska.
A pesar de estas estrategias en evolución, desde 2001 hasta 2021, las tasas de suicidio aumentaron la mayoría de los años, según los Centros para el Control y Prevención de Enfermedades (CDC). Los datos provisionales de 2022, los más recientes disponibles, muestran que las muertes por suicidio aumentaron un 3% adicional con respecto al año anterior.
Funcionarios de los CDC proyectan que el número final de suicidios en 2022 será aún mayor.
Pooja Mehta, defensora de la salud mental, con su hermano menor, Raj, que murió por suicidio en marzo de 2020. La muerte de Raj se produjo en medio de décadas de intentos infructuosos de reducir las tasas de suicidio en todo el país. “Hemos hecho un muy buen trabajo desarrollando soluciones para una parte del problema”, dijo Mehta. “Pero realmente no sabemos lo suficiente”.(Portia Eastman)
A pesar de esas cifras persistentemente desalentadoras, expertos en salud mental sostienen que las estrategias nacionales no son el problema. En cambio, argumentan que las políticas, por muchas razones, simplemente no se están financiando, adoptando y poniendo en marcha.
Esa lenta adopción se vio agravada por la pandemia de covid-19, que tuvo un amplio y negativo impacto en la salud mental.
Un grupo de expertos nacionales y funcionarios gubernamentales coincide en que las estrategias simplemente no han sido adoptadas de manera generalizada, y dijeron que incluso el seguimiento básico de las muertes por suicidio no es universal.
Los datos de vigilancia se utilizan comúnmente para impulsar la mejora de la calidad de la atención médica y han sido útiles para abordar el cáncer y las enfermedades cardíacas. Sin embargo, no se han utilizado en el estudio de problemas de salud conductual como el suicidio, dijo Michael Schoenbaum, asesor principal de servicios de salud mental, epidemiología y economía en el Instituto Nacional de Salud Mental (NIMH).
“Pensamos en tratar los problemas de salud conductual de manera diferente a como pensamos en los problemas de salud física”, dijo Schoenbaum.
Sin estadísticas precisas, los investigadores no pueden averiguar quién muere con mayor frecuencia por suicidio, qué estrategias de prevención están funcionando y dónde se necesita más dinero para la prevención.
Muchos estados y territorios no permiten que los registros médicos se vinculen a los certificados de defunción, dijo Schoenbaum, pero el NIMH está colaborando con otras organizaciones para documentar estos datos por primera vez en un informe público y una base de datos que se publicarán antes de fin de año.
Además, las estrategias enfrentan obstáculos en el hecho de que la financiación federal y local sube y baja, y algunos esfuerzos de prevención del suicidio no funcionan en ciertos estados y localidades debido a la geografía desafiante, dijo Jane Pearson, asesora especial de investigación sobre suicidio para el director del NIMH.
Wyoming, donde unos cientos de miles de residentes viven dispersos en un paisaje extenso y desigual, consistentemente se ubica entre los estados con las tasas más altas de suicidio.
Los funcionarios estatales han trabajado durante muchos años para abordar el problema del suicidio en el estado, dijo Kim Deti, portavoz del Departamento de Salud de Wyoming. Pero desplegar servicios, como unidades móviles de crisis, un elemento central de la estrategia nacional más reciente, es difícil en un estado grande y escasamente poblado.
“El trabajo no se detiene, pero algunas estrategias que tienen sentido en algunas áreas geográficas del país pueden no tenerlo en un estado con nuestras características”, dijo.
La falta de implementación no es solo un problema de los gobiernos estatales y locales. A pesar de la evidencia de que examinar a los pacientes en busca de pensamientos suicidas durante las visitas médicas ayuda a evitar catástrofes, no se obliga a los profesionales de la salud a hacerlo.
Lance Neiberger, voluntario del grupo de trabajo para la prevención del suicidio del condado de Natrona, muestra un marcador para niños con el número 988 de la línea directa de prevención de suicidio y crisis en Casper, Wyoming, el 14 de agosto de 2022.(Patrick T. Fallon/AFP via Getty Images)
Muchos médicos dicen que hacer las preguntas sobre el suicidio es desalentador porque tienen poco tiempo, una formación insuficiente y no se sienten cómodos hablando de suicidio, dijo Janet Lee, especialista en medicina adolescente y profesora asociada de pediatría en la Escuela de Medicina Lewis Katz de la Universidad Temple.
“Creo que es realmente aterrador y sorprendente pensar que si algo es una cuestión de vida o muerte, alguien no pueda preguntar sobre ello”, dijo.
El uso de otras medidas también ha sido inconsistente. Los servicios de intervención de crisis son fundamentales para las estrategias nacionales, pero muchos estados no han construido sistemas estandarizados.
Además de ser fragmentados, los sistemas de crisis, como las unidades móviles de crisis, pueden variar de un estado a otro y de un condado a otro. Algunas unidades móviles de crisis utilizan telemedicina, algunas operan las 24 horas del día y otras de 9 a 5, y algunas recurren a la policía local en lugar de buscar a trabajadores de salud mental.
Y la incipiente línea 988 de prevención del suicidio y crisis también enfrenta problemas graves.
Solo el 23% de los estadounidenses están familiarizados con el 988 y hay una brecha significativa de conocimiento sobre las situaciones en las que las personas deberían llamar al 988, según una encuesta reciente realizada por Ipsos y la Alianza Nacional sobre Afecciones Mentales.
La mayoría de los estados, territorios y naciones indígenas aún no han financiado de manera permanente al 988, que se lanzó a nivel nacional en julio de 2022 y ha recibido alrededor de $1,500 millones en fondos federales, según la Administración de Servicios de Salud Mental y Abuso de Sustancias (SAMHSA).
Anita Everett, directora del Centro de Servicios de Salud Mental de SAMHSA, dijo que su agencia está realizando una campaña de concientización para promover el sistema.
Algunos estados, como Colorado, están tomando otras medidas.
Allí, funcionarios estatales lanzaron incentivos financieros para implementar esfuerzos de prevención del suicidio, entre otras medidas de seguridad para los pacientes, a través del Programa Estatal de Pago por Incentivos de Calidad Hospitalaria.
El programa otorga alrededor de $150 millones al año a los hospitales por su buen desempeño. En el último año, 66 hospitales mejoraron su atención a los pacientes que tuvieron conductas suicidas, según Lena Heilmann, directora de la Oficina de Prevención del Suicidio del Departamento de Salud Pública y Medio Ambiente de Colorado.
Los expertos esperan que otros estados sigan el ejemplo de Colorado.
Y a pesar del lento avance, Mehta ve puntos positivos en la última estrategia y plan de acción. Aunque es demasiado tarde para salvar a Raj, “abordar los factores sociales que impulsan la salud mental y el suicidio e invertir en espacios para que las personas busquen ayuda mucho antes de una crisis me da esperanza”, dijo Mehta.
El reportaje de Cheryl Platzman Weinstock cuenta con el apoyo de una beca del National Institute for Health Care Management Foundation.
Esta historia fue producida por KFF Health News, conocido antes como Kaiser Health News (KHN), una redacción nacional que produce periodismo en profundidad sobre temas de salud y es uno de los principales programas operativos de KFF, la fuente independiente de investigación de políticas de salud, encuestas y periodismo.
SIKESTON, Mo. — I wasn’t sure if visiting a cotton field was a good idea. Almost everyone in my family was antsy when we pulled up to the sea of white.
The cotton was beautiful but soggy. An autumn rain had drenched the dirt before we arrived, our shoes sinking into the ground with each step. I felt like a stranger to the soil.
My daughter, Lily, then 5, happily touched a cotton boil for the first time. She said it looked like mashed potatoes. My dad posed for a few photos while I tried to take it all in. We were standing there — three generations strong — on the edge of a cotton field 150 miles away from home and decades removed from our own past. I hoped this was an opportunity for us to understand our story.
As a journalist, I cover the ways racism — including the violence that can come with it — can impact our health. For the past few years, I’ve been working on a documentary film and podcast called “Silence in Sikeston.” The project is about two killings that happened decades apart in this Missouri city: a lynching in 1942 of a young Black man named Cleo Wright and a 2020 police shooting of another young Black man, Denzel Taylor. My reporting explored the trauma that festered in the silence around their killings.
While I interviewed Black families to learn more about the effect of these violent acts on this rural community of 16,000, I couldn’t stop thinking about my own family. Yet I didn’t know just how much of our story, and the silence surrounding it, echoed Sikeston’s trauma. My father revealed our family’s secret only after I delved into this reporting.
My daughter was too young to understand our family’s past. I was still trying to understand it, too. Instead of trying to explain it right away, I took everyone to a cotton field.
Cotton is complicated. White people got rich off cotton while my ancestors received nothing for their enslaved labor. My grandparents then worked hard in those fields for little money so we wouldn’t have to do the same. But my dad still smiled when he posed for a picture that day in the field.
“I see a lot of memories,” he said.
Wilbon Anthony, Cara Anthony’s father, poses for a portrait with a cotton plant on Oct. 3, 2021, in Sikeston, Missouri.(Michael B. Thomas for KFF Health News)
I’m the first generation to never live on a farm. Many Black Americans share that experience, having fled the South during the Great Migration of the last century. Our family left rural Tennessee for cities in the Midwest, but we rarely talked about it. Most of my cousins had seen cotton fields only in movies, never in real life. Our parents worked hard to keep things that way.
At the field that day, my mom never left the van. She didn’t need to see the cotton up close. She was around Lily’s age when her grandfather taught her how to pick cotton. He had a third-grade education and owned more than 100 acres in western Tennessee. Sometimes she had to stay home from school to help work that land while her peers were in class. She would watch the school bus pass by the field.
“I would just hide, lying underneath the cotton stalks, laying as close to the ground as I could, trying to make sure that no one would see me,” my mom said. “It was very embarrassing.”
She didn’t talk to me about that part of her life until we traveled to Sikeston. Our trip to the cotton field opened the door to a conversation that wasn’t easy but was necessary. My reporting sparked similar hard conversations with my dad.
Subscribe to California Healthline’s free Daily Edition.
As a child, I overheard adults in my family as they discussed racism and the art of holding their tongues when a white person mistreated them. On my mother’s side of the family, when we’d gather for the holidays, aunts and uncles discussed cross-burnings in the South and in the Midwest. Even in the 1990s, someone placed a burning cross outside a school in Dubuque, Iowa, where one of my relatives served as the city’s first Black principal.
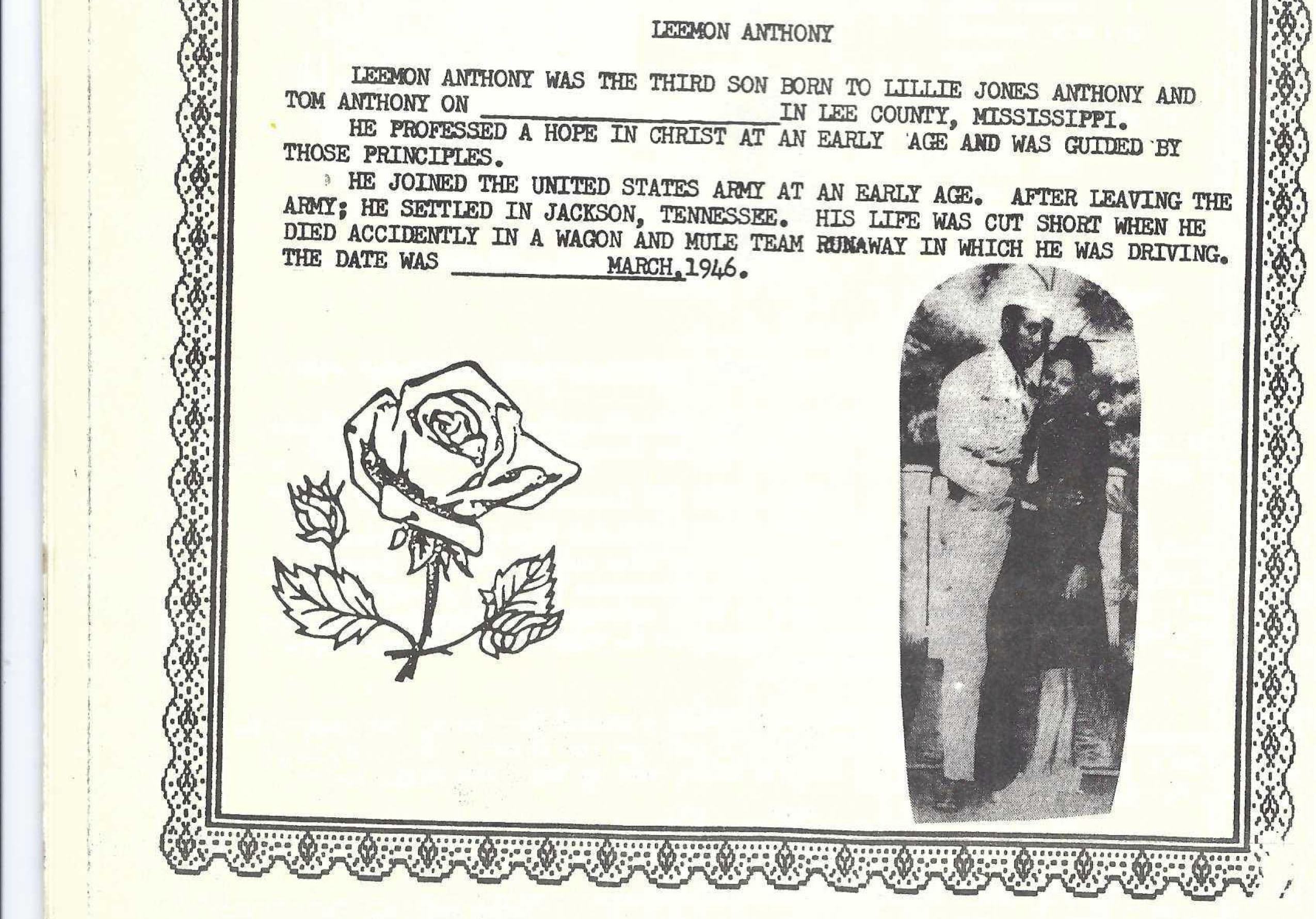
On my father’s side of the family, I heard stories about a relative who died young, my great-uncle Leemon Anthony. For most of my dad’s life, people had said my great-uncle died in a wagon-and-mule accident.
“There was a hint there was something to do with it about the police,” my dad told me recently. “But it wasn’t much.”
So, years ago, my dad decided to investigate.
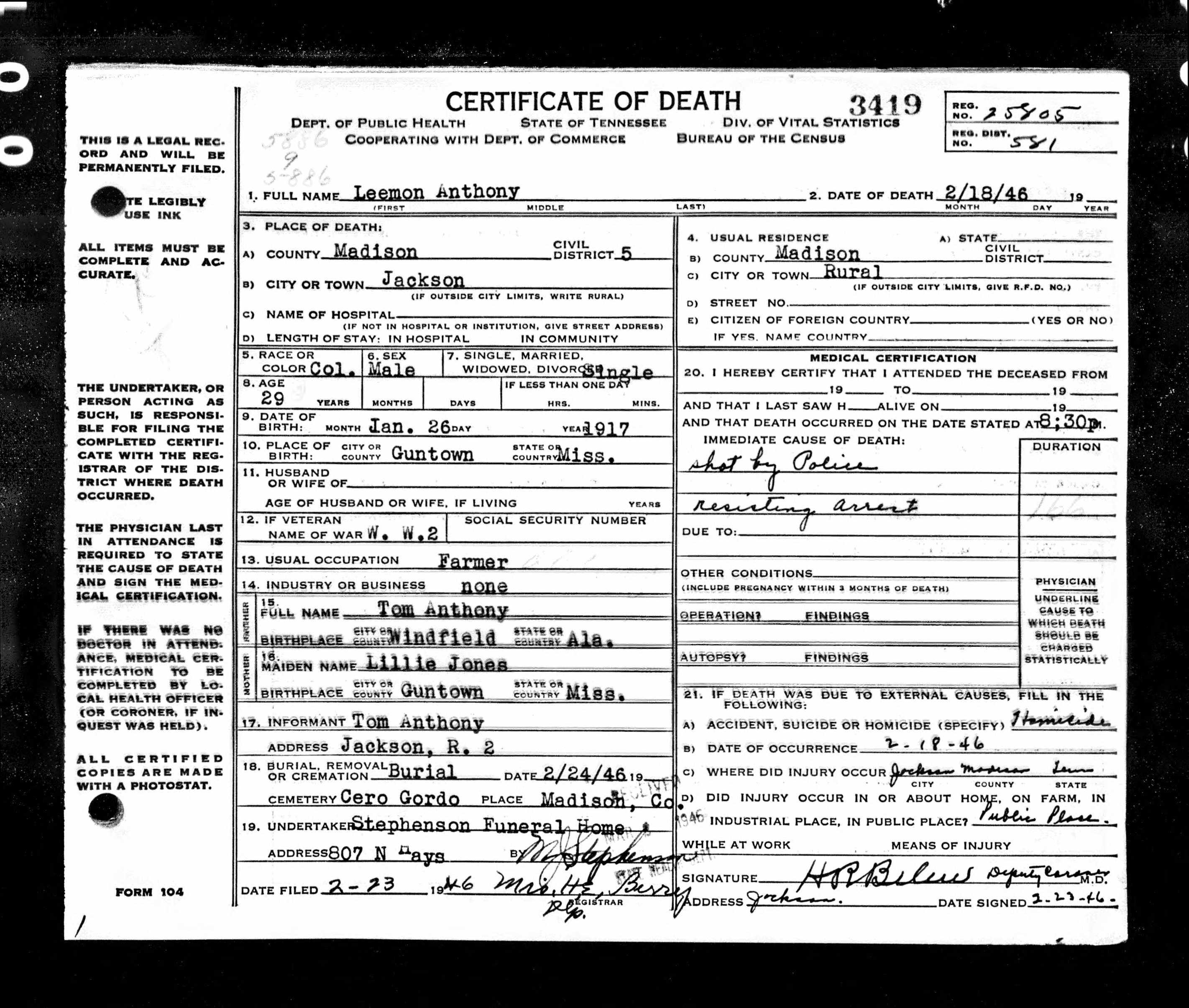
He called up family members, dug through online newspaper archives, and searched ancestry websites. Eventually, he found Leemon’s death certificate. But for more than a decade, he kept what he found to himself — until I started telling him about the stories from Sikeston.
“It says ‘shot by police,’ ‘resisting arrest,’” my dad explained to me in his home office as we looked at the death certificate. “I never heard this in my whole life. I thought he died in an accident.”
Leemon’s death in 1946 was listed as a homicide and the officers involved weren’t charged with any crime. Every detail mirrored modern-day police shootings and lynchings from the past.
A page from a 1986 Anthony family reunion booklet shows an image of Leemon Anthony. The World War II veteran was killed in 1946 by a police officer in Tennessee.(The Anthony family)A police officer in Tennessee killed Leemon Anthony in 1946, according to his death certificate.(Tennessee Death Records/Tennessee State Library Archives)
This young Black man — whom my family remembered as fun-loving, outgoing, and handsome — was killed without any court trial, as Taylor was when police shot him and Wright was when a mob lynched him in Sikeston. Even if the men were guilty of the crimes that prompted the confrontations, those allegations would not have triggered the death penalty.
At a hearing in 1946, a police officer said that he shot my uncle in self-defense after Leemon took the officer’s gun away from him three times during a fight, according to a Jackson Sun newspaper article my dad found. In the article, my great-grandfather said that Leemon had been “restless,” “absent minded,” and “all out of shape” since he returned home from serving overseas in the Army during World War II.
Before I could ask any questions, my dad’s phone rang. While he looked to see who was calling, I tried to gather my thoughts. I was overwhelmed by the details.
My dad later gently reminded me that Leemon’s story wasn’t unique. “A lot of us have had these incidents in our families,” he said.
Our conversation took place when activists around the world were speaking out about racial violence, shouting names, and protesting for change. But no one had done that for my uncle. A painful piece of my family’s story had been filed away, silenced. My dad seemed to be the only one holding space for my great-uncle Leemon — a name that was no longer spoken. Yet my dad was doing it alone.
It seems like something we should have discussed as a family. I wondered how it shaped his view of the world and whether he saw himself in Leemon. I felt a sense of grief that was hard to process.
Wiliam Avery, Lorenzie Avery, Cara Anthony, and Cara’s mother stand outside the family’s home in East St. Louis, Illinois. Lorenzie’s brother, Leemon Anthony, was killed after an altercation with a police officer in 1946. (The Anthony family)
Cara Anthony’s family stands together for a photo in the early ’90s. (The Anthony family)
So, as part of my reporting on Sikeston, I spoke to Aiesha Lee, a licensed counselor and Penn State University assistant professor who studies intergenerational trauma.
“This pain has compounded over generations,” Lee said. “We’re going to have to deconstruct it or heal it over generations.”
Lee said that when Black families like mine and those in Sikeston talk about our wounds, it represents the first step toward healing. Not doing so, she said, can lead to mental and physical health problems.
In my family, breaking our silence feels scary. As a society, we’re still learning how to talk about the anxiety, stress, shame, and fear that come from the heavy burden of systemic racism. We all have a responsibility to confront it — not just Black families. I wish we didn’t have to deal with racism, but, in the meantime, my family has decided not to suffer in silence.
On that same trip to the cotton field, I introduced my dad to the families I’d interviewed in Sikeston. They talked to him about Cleo and Denzel. He talked to them about Leemon, too.
I wasn’t thinking about my great-uncle when I first packed my bags for rural Missouri to tell the stories about other Black families. But my dad was holding on to Leemon’s story. By keeping the file — and finally sharing it with me — he was making sure his uncle was remembered. Now I say each of their names: Cleo Wright. Denzel Taylor. Leemon Anthony.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
WINDER, Ga. — About an hour after gunfire erupted at Apalachee High School, ambulances started arriving at nearby Northeast Georgia Medical Center Barrow with two students and two adults suffering from panic attacks and extreme anxiety, not bullet wounds.
A fifth patient with similar symptoms later arrived at another local facility, according to a health system spokesperson.
The day after the Sept. 4 school shooting that killed two students and two teachers, some 80 families showed up in a county office to receive counseling from volunteer therapists who converged from across the Atlanta metro area, according to one medical provider. That Sunday, nine people received free treatment at a local church for post-traumatic stress disorder from volunteering Atlanta-area providers. On Monday, the state opened a temporary recovery center to help locals find counseling, faith-based support, or other aid. The needs are still great.
“We don’t really know how we’re doing,” Amanda McKee — whose son, Asa Deslonde, is a senior at Apalachee — said two days after the shooting. “It’s second by second. It’s minute by minute. The last couple days have been unimaginable.”
Apalachee High School remained closed in the days after the Sept. 4 shooting there that left four people dead. Many mental health advocates worry whether the Georgia community will receive the mental health support it is likely to need in the wake of the shooting.(Andy Miller for KFF Health News)
When shootings of any magnitude occur, they often leave the survivors with invisible injuries that can create life-changing symptoms that sometimesparalyze them.But such problems can take time to emerge. Panic attacks and anxiety can spike across a community after a shooting and can be most intense when people return to the scene, said Howard Liu, chair of the Council on Communications for the American Psychiatric Association.
So health providers worry that in the coming days, months, and years the community will struggle to find help for their mental health needs. Barrow County, along a highway that connects Atlanta to the college town of Athens, is a community where agriculture is steadily giving way to development.
Prior to the shooting, the area had one stand-alone inpatient mental health facility, located in Gainesville, about 30 miles away from where the shooting occurred in Barrow County, that was “constantly overwhelmed,” said Sean Couch, a spokesperson for Northeast Georgia Health System. And, the latest federal data shows, Barrow would need to add at least 13 full-time providers to no longer be considered a mental health workforce shortage area.
“We put a band-aid on a chronic situation and that band-aid isn’t going to last,” said Roland Behm, a co-founder of the Georgia Mental Health Policy Partnership, an advocacy group that represents mental health organizations in the state. “What happens three months from now?”
Subscribe to California Healthline’s free Daily Edition.
The scarcity of mental health providers in Barrow County is emblematic of the state as a whole. Georgia ranks nearly last among states in access to mental health care resources, according to Mental Health America, a nonprofit that advocates for increased mental health spending. More than 5 million Georgians live in mental health care professional shortage areas like Barrow County.
Paying for mental health care to treat such trauma is difficult nationwide. But Georgia is one of the 10 states that have not fully expanded eligibility for Medicaid, the nation’s safety net insurance for those with low incomes and also the largest payer for mental health services. The state has an uninsured rate of 13.6%, which is 4.1 percentage points higher than the country as a whole, according to 2022 data from the U.S Census Bureau.
Even people with private health plans have trouble finding affordable, in-network mental health care because of a lack of providers willing to accept low insurance reimbursement rates, Behm said.
Tamara Conlin, CEO of Advantage Behavioral Health Systems, said the people who came to the initial counseling sessions that her group helped arrange in a county office showed a lot of sadness and anxiety.
“Some of them are still in shock and trying to wrap their heads around what happened,” she said.
Even before the shooting, students at Apalachee High School reported significant mental health challenges.
Nearly 200 of 1,725 student respondents reported that they had seriously considered attempting suicide one or more times in the prior year, according to the latest Georgia Student Health Survey. Top motivators included problems with peers, friends, or family. About half of the students from the school who answered said they felt sad, depressed, or withdrawn at least once in the prior 30 days.
County residents complained about having to travel for psychiatric care and said the “shortage of psychologists and counseling services led to untreated high anxiety and depression rates,” during a 2019 focus group about health care access.
The lack of mental health care remained a top concern in the region during a follow-up assessment in 2022. That year, the opioid overdose death rate in Barrow County was among the highest in Georgia, according to state data, and the five-year suicide rate was above the state average.
The Barrow County School System, which includes Apalachee High School, received a $1.8 million federal grant to boost mental health resources in schools from 2023 through 2028.
But immediately following the shooting, mental health providers across the region still had to cobble together free resources for area residents. Three volunteers helped with last Wednesday’s response at Northeast Georgia Medical Center Barrow. Advantage Behavioral Health Systems kept its Barrow clinic open on Sunday and is providing counselors to community events and local schools as they reopen.
William Smith, who heads the Atlanta Center for EMDR, is planning sessions using eye movement desensitization and reprocessing therapy to address PTSD — at least one for first responders and another for residents.
Over the weekend, Lutheran Church Charities brought nine golden retrievers as “comfort dogs” to help the grieving. The group’s dogs have been deployed in the wake of other school shootings, including the Uvalde, Texas, massacre.
Phinehas is one of several “comfort dogs” brought by Lutheran Church Charities to Winder, Georgia, to help grieving community members and students in the wake of the Apalachee school shooting on Sept. 4. The dogs came from six states, including Nebraska, where Phinehas lives.(Andy Miller for KFF Health News)
“We can’t fix what they’re feeling,” said volunteer Paul Soost, as people gathered around a campus flagpole where they delivered flowers and messages. “We can provide comfort.”
Many health care providers expect the community’s needs to spike when students return to Apalachee High School and as the national attention on the shooting recedes.
“That’s when people start experiencing the trauma,” said Conlin, with Advantage Behavioral Health Systems, who compared the current crisis to the surge of patients she saw after the immediate threat of the covid-19 pandemic passed.
Her clinic in Barrow County already had about 750 active clients before the shooting, with about 120 under the age of 18.
McKee said she knows healing will be a long process for her son, Asa. One of his football coaches, Richard Aspinwall, was among the four killed. A key step came the day after the shooting, she said, when the school’s head football coach convened the team to share how much he was hurting.
“The coach validated that they were hurt, and encouraged them to embrace that they were injured,” McKee said. “They’re not the physical injuries that were incurred by the senseless act, but they are injuries nonetheless.”
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
If you or someone you know may be experiencing a mental health crisis, contact the 988 Suicide & Crisis Lifeline by dialing or texting “988.”
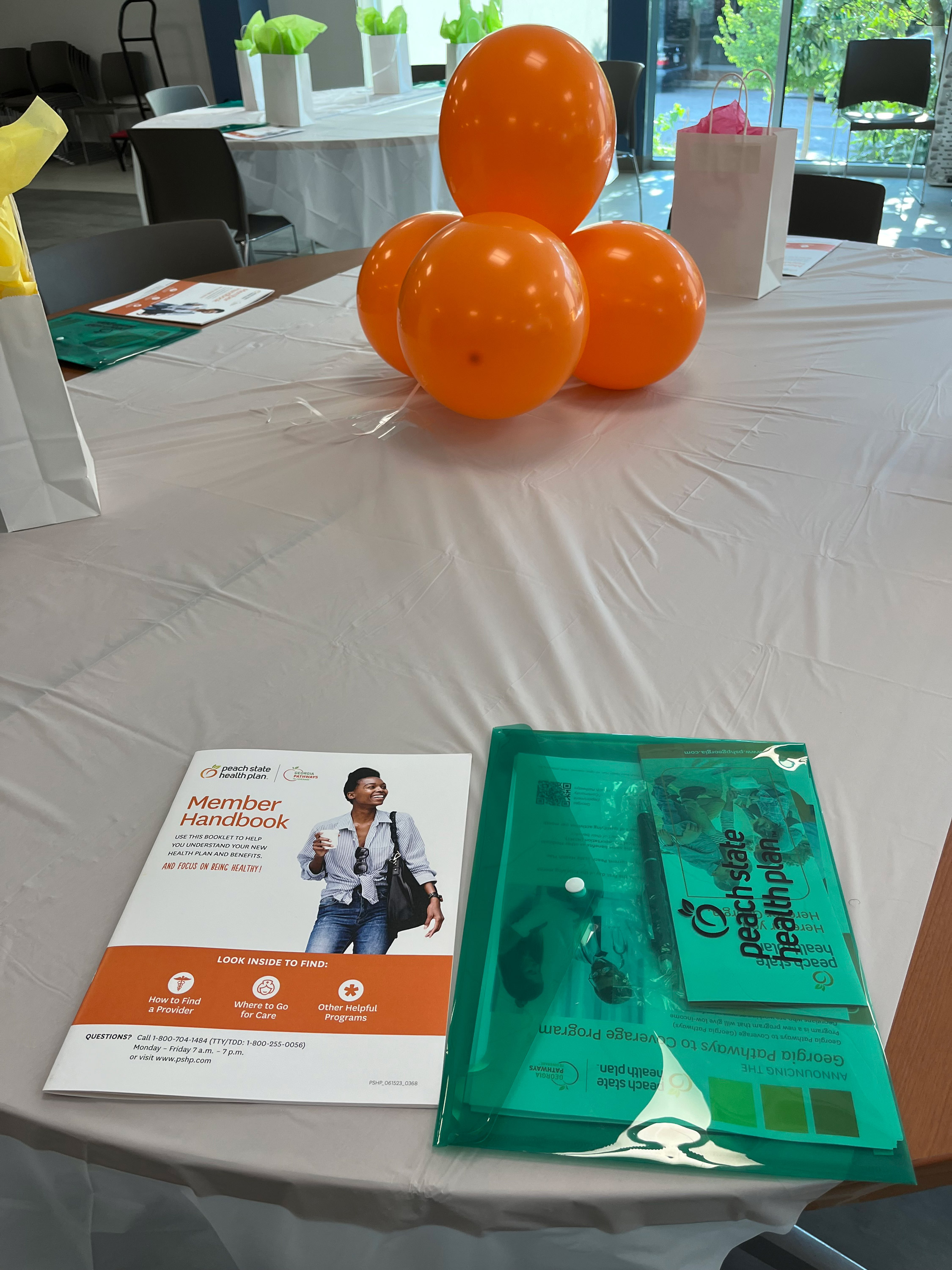
ATLANTA — On a recent summer evening, Raymia Taylor wandered into a recreation center in a historical downtown neighborhood, the only enrollee to attend a nearly two-hour event for people who have signed up for Georgia’s experimental Medicaid expansion.
The state launched the program in July 2023, requiring participants to document that they’re working, studying, or doing other qualifying activities for 80 hours a month in exchange for health coverage. At the event, booths were set up to help people join the Marines or pursue a GED diploma.
Taylor, 20, already met the program’s requirements — she studies nursing and works at a fast-food restaurant. But she said it wasn’t clear what paperwork to submit or how to upload her documents. “I was struggling,” she said.
Georgia is the only state that requires certain Medicaid beneficiaries to work to get coverage. Republicans have long touted such programs, arguing they encourage participants to maintain employment. About 20 states have applied to enact Medicaid work requirements; 13 won approval under the Trump administration. The Biden administration has worked to block such initiatives.
The Georgia Pathways to Coverage program shows the hurdles ahead for states looking to follow its lead. Georgia’s GOP leaders have spent millions of dollars to launch Pathways. By July 29, nearly 4,500 people had enrolled, the state’s Medicaid agency told KFF Health News.
That’s well short of the state’s own goal of more than 25,000 in its first year, according to its application to the federal government, and a fraction of the 359,000 who might have been eligible had Georgia simply expanded Medicaid under the Affordable Care Act, as 40 other states did.
So far, the pricey endeavor has forced participants to navigate bureaucratic hurdles rather than support employment. The state would not confirm whether it could even verify if people in the program are working.
Only one enrollee attended a nearly two-hour event for people in Georgia’s experimental Medicaid program, which requires participants to document that they’re working, studying, or performing other qualifying activities for 80 hours a month in exchange for health coverage. At the event, booths were set up to help people join the Marines or pursue a GED diploma.(Renuka Rayasam/KFF Health News)
Research shows such red tape disproportionately affects Black and Hispanic people.
“The people that need access to health care coverage the most are going to struggle with that administrative burden because the process is so complicated,” said Leah Chan, director of health justice at the Georgia Budget and Policy Institute.
At an August press event, Georgia Republican Gov. Brian Kemp announced a $10.7 million ad campaign to boost enrollment in Pathways, one of his administration’s major health policy initiatives. The plan has cost more than $40 million in state and federal tax dollars through June, with nearly 80% going toward administration and consulting fees rather than paying for medical care, according to data the state Medicaid agency shared with KFF Health News.
Enrollment advisers, consumer advocates, and policy researchers largely blame a cumbersome enrollment process, complicated program design, and back-end technology flaws for Pathways’ flagging enrollment. They say that the online application is challenging to navigate and understand and lacks a way for people to receive immediate support, and that state staffers don’t respond to applicants in a timely manner.
“It’s just an administrative nightmare,” said Cynthia Gibson, director of the Georgia Legal Services Program’s Health Law Unit, who helps Pathways applicants appeal denials.
Administrative challenges have also undermined a key part of the program’s philosophy: that people maintain employment to keep coverage. As of July, the state was not removing enrollees for not meeting Pathways’ work requirement, according to Fiona Roberts, a spokesperson for Georgia’s Medicaid agency.
“We understand that people need to be held accountable to those 80 hours for the spirit of the program, and we intend to do that,” said Russel Carlson, the agency’s commissioner.
Pathways is set to expire Sept. 30, 2025, unless the state asks the Centers for Medicare & Medicaid Services for an extension. Georgia officials say they won’t have to make that request until next spring, well after November’s election. So the state could be asking for an extension from the Trump administration, which approved the program in the first place.
Georgia officials sued the Biden administration this year to keep Pathways running without going through the official extension process, which requires the state to conduct public comment sessions, gather extensive financial data, and prove that Pathways has met its goals. A federal judge ruled against Georgia.
A CMS spokesperson said the agency wouldn’t comment on the program.
During the August press event, Kemp said the Biden administration’s attempt to stop the program in 2021 delayed its rollout and stymied enrollment. A federal court blocked the administration and allowed Georgia to proceed.
People familiar with the enrollment process said Pathways has been mired in design flaws and system failures. As of the end of May, 13,702 applications were waiting to be processed, according to state documents.
The program’s lengthy questionnaires and technical language are confusing, guidance is opaque, and tools to upload documents are tricky to navigate, according to interviews with health insurance enrollment specialists conducted for the Georgia Budget and Policy Institute.
“It’s not an easy, ‘Oh, I want to apply for Pathways,’” said Deanna Williams, who helps people enroll in insurance plans at Georgians for a Healthy Future, a consumer advocacy group. People generally learn about the program after being denied other Medicaid coverage, she said.
In the online application, people click through pages of questions before they’re shown a screen with information about Pathways, Williams said. Then they must check a box and sign a form saying they understand the program’s requirements.
Sometimes the Pathways application doesn’t pop up, and she must start over. The process to apply is “not smooth,” she said.
Data shows that people who don’t earn enough to qualify for free ACA plans but also make too much for Medicaid are disproportionately people of color. Pathways offers Medicaid coverage to adults earning up to the federal poverty level: $15,060 for an individual or $31,200 for a family of four.
Some people eligible for Pathways who work in retail or restaurants with fluctuating hours are nervous they can’t meet requirements every month, Williams said.
Many current enrollees don’t know how to upload documents, and the website sometimes stops working, said Jahan Becham, an employment specialist for Pathways at Amerigroup Community Care. Or people just forget.
Every month Becham gets a list of 200 to 300 enrollees who haven’t submitted their hours. “It is something new, and not many people are used to this,” Becham said.
“I would get reminders,” said Taylor, who attended the event for enrollees in August. “I just didn’t know how.”
In a June 2023 meeting with Georgia Medicaid staffers weeks before the program launched, federal officials questioned why the state wasn’t automatically verifying eligibility with existing data sources, according to meeting minutes KFF Health News obtained through a state open-records request. Georgia officials said they were unsure when they’d be able to simplify the verification process.
Many potential participants face improper denials, advocates said. Gibson, at the Georgia Legal Services Program, said not enough workers are trained to properly evaluate applications.
Fewer than 1 in 5 people who have their Pathways applications processed had been accepted into the program as of May, according to a KFF Health News analysis of state data. Roberts, with the state, said people were denied because they earned too much, didn’t meet requirements, or didn’t complete the paperwork.
A full-time graduate student was wrongly blocked from the program, and in February a state administrative judge ordered her case be reconsidered. In another case, a different judge ruled a 64-year-old woman who couldn’t work because she was her disabled husband’s full-time caregiver would not qualify for Pathways.
Despite the challenges, state records from May show no individuals were removed from the program since it launched for failing to meet work requirements.
Georgia’s experiment comes after a 2018 effort in Arkansas to implement work requirements on an existing Medicaid expansion population led to 18,000 people losing coverage, many of whom either met requirements or would have been exempted.
Taylor found out about Pathways when she applied for food stamps last year. It wasn’t until August that she learned she could submit her school schedule to meet the qualifying hours requirement. With a full Medicaid expansion, Taylor would have been eligible for health coverage without the extra effort. But, for her, it’s still worth it.
“It’s important to have health insurance,” said Taylor, who has been to the dentist several times and plans to visit a doctor. “I’m glad I have it.”
As expected, the presidential debate between former President Donald Trump and Vice President Kamala Harris offered few new details of their positions on abortion, the Affordable Care Act, and other critical health issues. But it did underscore for voters dramatic differences between the two candidates.
Meanwhile, the Biden administration issued rules attempting to better enforce mental health parity — the federal government’s requirement that services for mental health care and substance use disorders be covered by insurance to the same extent as other medical services.
This week’s panelists are Julie Rovner of KFF Health News, Rachel Cohrs Zhang of Stat, Riley Griffin of Bloomberg News, and Lauren Weber of The Washington Post.
Among the takeaways from this week’s episode:
Trump declined to say during the debate whether he’d veto legislation implementing a nationwide abortion ban. But he could effectively ban the procedure without Congress passing anything because of the 150-year-old Comstock Act. And Project 2025, a policy blueprint by the conservative Heritage Foundation, calls for doing just that.
There is a good chance that enhanced federal subsidies for ACA coverage that were introduced during the pandemic could expire next year, depending on which party controls Congress. The subsidies have helped more people secure zero-premium health coverage through the ACA exchanges, though Republicans say the subsidies cost too much to keep. Residents in states that haven’t expanded Medicaid coverage — including Florida and Texas — would be most affected.
The Census Bureau reports that the uninsured rate didn’t change much last year after hitting a record low in the first quarter. But the report’s methodology prevented it from capturing the experiences of many people disenrolled and left uninsured after what’s known as the Medicaid “unwinding” began. Meanwhile, a Treasury Department report sheds light on just how many Americans have benefited from the ACA, as polls show the health law has also grown more popular.
And Congress has yet to pass key government spending bills, meaning the nation (again) faces a possible federal government shutdown starting Oct. 1. It remains to be seen what could pass during a lame-duck session after the November elections. In 2020, the end-of-the-year spending package featured many health care priorities — and that could happen again.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.