Hospitals around the country are conserving critical intravenous fluid supplies to cope with a shortage that may last months. Some hospital administrators say they are changing how they think about IV fluid hydration altogether.
Hurricane Helene, which hit North Carolina in September, wrecked a Baxter International facility that produces 60% of the IV fluids used in the U.S., according to the American Hospital Association.
The company was forced to stop production and is rationing its products. In an update posted Nov. 7, Baxter said its North Cove facility had resumed producing some IV fluids. In an email to KFF Health News, the company wrote that customers will be able to order normal quantities of “certain IV solutions products” by the end of the year, but there is no timeline for when the North Cove facility will be back to prehurricane production levels.
Meanwhile, hospitals are facing seasonal strains on their already limited IV fluid resources, said Sam Elgawly, chief of resource stewardship at Inova, a health system in the Washington, D.C., area.
“We’ve been very aggressive in our conservation measures,” Elgawly said, stressing that he does not believe patient care has been compromised. He told KFF Health News that across the system IV fluid usage has dropped 55% since early October.
Elgawly called the shortage a crisis that he expects to have to continue managing for some time. “We are going to operate under the assumption that this is going to be the way it is through the end of 2024 and have adopted our demand/conservation measures accordingly,” he said.
Subscribe to California Healthline’s free Daily Edition.
At the end of the calendar year, many patients with insurance hurry to schedule surgical procedures before their deductibles reset in January. Elgawly is eyeing that typical surgical rush and the impending peak of respiratory virus season as he tries to stockpile IV fluid bags. Hospitals such as Inova’s are using different ways to conserve, such as giving some medications intravenously, but without a dedicated IV fluid bag, known as a push medication.
“You don’t even need a bag at all. You just give the medication without the bag,” he said. “There has been increasing literature over the last 10 to 20 years that indicates maybe you don’t need to use as much. And this accelerated our sort of innovation and testing of that idea.”
Monica Coleman is a nurse at a Department of Veterans Affairs hospital in North Chicago. She said using push medications takes more time out of a nurse’s already hectic schedule because then they need to monitor the patient.
“This could increase adverse effects within the patient, because we’re giving the medication at a faster rate,” she said.
Elgawly is also interested in retooling electronic health records to question doctor orders for more IV hydration.
“Does the patient actually need that second bag? How did they do today with eating or drinking water or juice? They did well? They don’t need the bag. So it’s little conservation mechanisms like that that, when you add them across, you know, the 2,000-patient system that Inova is, make a significant dent,” he said.
Simpler conservation measures could become common after the shortage abates, said Vince Green, chief medical officer for Pipeline Health, a small hospital system in the Los Angeles area that serves mainly people on Medicare and Medicaid.
First, Green would like to see data showing that patient outcomes aren’t affected. But for now, some of the new strategies just make sense to him. He has directed hospital staff to use up the entire IV bag before starting another.
“If they come in with IV fluids that the paramedics have started, let’s continue it. If it saves half a bag of fluids, so be it, but it adds up over time,” he said.
Patients may be asked to take more accountability for their hydration, by drinking Gatorade or water rather than the default of hydrating through an IV, he said.
“From an environmental aspect, we don’t need to have this much waste and fill up our landfills. If we could reduce stuff, I think it’d be wise,” he said.
But he’ll feel better when his hospitals receive a full order, which could be weeks away. Green said they are down to a two-week supply, with an expected increase in hospitalizations due to respiratory virus season.
“We’re purchasing every IV fluid bag that we can get,” he said.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
Study Identifies Pregnant Women at Risk for Substance Use
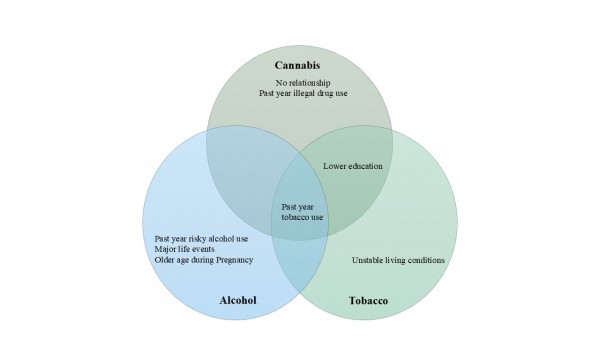
STONY BROOK, NY, November 18, 2024 – Use of tobacco, alcohol, cannabis, and illicit drugs is dangerous in pregnancy, increasing risks of stroke, miscarriage, preterm delivery, low birth weight and infant neurodevelopmental problems. Yet according to the 2020 National Survey of Drug Use and Health, more than 20 percent of pregnant women in the United States report using one or more of these substances. Public health experts agree on the need to identify pregnant women who are most vulnerable to using harmful substances. A new study published in the Journal of Addiction Medicine conducted by a team of Stony Brook University researchers used the PROMOTE Prenatal Screener – a unique screening tool for use during pregnancy – to pinpoint vulnerabilities for substance use.
The study, led by Heidi Preis, MSW, PhD, Assistant Professor of Research in the Department of Obstetrics, Gynecology and Reproductive Medicine in the Renaissance School of Medicine (RSOM), focused on vulnerabilities for tobacco, cannabis, or alcohol use in pregnancy.
“When patients complete the PROMOTE at the start of their prenatal care, their health care providers can identify any psychological, social, or other needs and determine whether a particular patient is likely to use harmful substances during pregnancy,” explains Preis, who also has academic affiliations and collaborates with Stony Brook’s Program in Public Health and Department of Psychology. “This way a patient’s needs can be addressed very early and she can be referred for counseling, treatment, or resources, and this reduces harms for both mother and child.”
Preis and colleagues developed the PROMOTE with a grant from the National Institutes of Health’s National Institute on Drug Abuse (NIDA). Prior to its creation, a comprehensive yet concise screening tool to detect psychosocial and substance use risk was not available in prenatal care settings. The PROMOTE includes 18 core items that address vulnerabilities in areas such as education, financial stability, living conditions, partner and family stress and support, exposure to violence, and mental health.
For their current study, the team reviewed medical charts of 1,842 patients who completed the PROMOTE during their first prenatal visit to a New York State health system outpatient clinic. They found that 188 patients (10.2%) used at least one substance during pregnancy, including 132 (7.2%) tobacco, 50 (2.7%) cannabis, and 45 (2.4%) alcohol. Patients with limited education were most likely to use tobacco during pregnancy, single and unpartnered patients were most likely to use cannabis, and those who experienced a major stressful life event were most likely to use alcohol during pregnancy. Other vulnerabilities were also associated with harmful substance use.
Their study results highlight the value of using a well-developed screening tool to gain a better understanding of the life context of pregnant patients and identify those who are most vulnerable or might be struggling with substance use. Preis stresses that addressing their needs has great potential to improve the health and well-being of pregnant women and their children.
Co-authors and collaborators on the PROMOTE project include: Marci Lobel, PhD, Department of Psychology and Department of Obstetrics, Gynecology and Reproductive Medicine; Cassandra Heiselman, DO, Department of Obstetrics, Gynecology and Reproductive Medicine; Ayesha Azeem, RSOM student and first author of the publication; David Garry, MD, Department of Obstetrics, Gynecology and Reproductive Medicine.
Study Identifies Pregnant Women at Risk for Substance Use
STONY BROOK, NY, November 18, 2024 – Use of tobacco, alcohol, cannabis, and illicit drugs is dangerous in pregnancy, increasing risks of stroke, miscarriage, preterm delivery, low birth weight and infant neurodevelopmental problems. Yet according to the 2020 National Survey of Drug Use and Health, more than 20 percent of pregnant women in the United States report using one or more of these substances. Public health experts agree on the need to identify pregnant women who are most vulnerable to using harmful substances. A new study published in the Journal of Addiction Medicine conducted by a team of Stony Brook University researchers used the PROMOTE Prenatal Screener – a unique screening tool for use during pregnancy – to pinpoint vulnerabilities for substance use.
The study, led by Heidi Preis, MSW, PhD, Assistant Professor of Research in the Department of Obstetrics, Gynecology and Reproductive Medicine in the Renaissance School of Medicine (RSOM), focused on vulnerabilities for tobacco, cannabis, or alcohol use in pregnancy.
“When patients complete the PROMOTE at the start of their prenatal care, their health care providers can identify any psychological, social, or other needs and determine whether a particular patient is likely to use harmful substances during pregnancy,” explains Preis, who also has academic affiliations and collaborates with Stony Brook’s Program in Public Health and Department of Psychology. “This way a patient’s needs can be addressed very early and she can be referred for counseling, treatment, or resources, and this reduces harms for both mother and child.”
Preis and colleagues developed the PROMOTE with a grant from the National Institutes of Health’s National Institute on Drug Abuse (NIDA). Prior to its creation, a comprehensive yet concise screening tool to detect psychosocial and substance use risk was not available in prenatal care settings. The PROMOTE includes 18 core items that address vulnerabilities in areas such as education, financial stability, living conditions, partner and family stress and support, exposure to violence, and mental health.
For their current study, the team reviewed medical charts of 1,842 patients who completed the PROMOTE during their first prenatal visit to a New York State health system outpatient clinic. They found that 188 patients (10.2%) used at least one substance during pregnancy, including 132 (7.2%) tobacco, 50 (2.7%) cannabis, and 45 (2.4%) alcohol. Patients with limited education were most likely to use tobacco during pregnancy, single and unpartnered patients were most likely to use cannabis, and those who experienced a major stressful life event were most likely to use alcohol during pregnancy. Other vulnerabilities were also associated with harmful substance use.
Their study results highlight the value of using a well-developed screening tool to gain a better understanding of the life context of pregnant patients and identify those who are most vulnerable or might be struggling with substance use. Preis stresses that addressing their needs has great potential to improve the health and well-being of pregnant women and their children.
Co-authors and collaborators on the PROMOTE project include: Marci Lobel, PhD, Department of Psychology and Department of Obstetrics, Gynecology and Reproductive Medicine; Cassandra Heiselman, DO, Department of Obstetrics, Gynecology and Reproductive Medicine; Ayesha Azeem, RSOM student and first author of the publication; David Garry, MD, Department of Obstetrics, Gynecology and Reproductive Medicine.
Race influences the treatments of opioid use disorders.
There is an opioid crisis and a health disparities crisis.
Racial equity should include increasing access for treatment, funding harm reduction programs and expanding community-based services such as employment, housing, and recovery support for those with opioid use disorder.
ANALYSIS
Background
The United States listed the opioid crisis as a public health emergency (1). Concurrently, the United States has a racial health disparities crisis that is evident as patients from various races receive different health care treatments (2). The opioid crisis has impacted all racial groups, with incidence rates of 11.9, 9.3%, and 9.6% in the White, Black, and Hispanic populations, respectively(3).
Multiple studies have listed that racial disparities in pain treatment are associated with lower opioid use in minority patients during the beginning of liberalized opioid use in clinical settings (4). Disparities in pain treatment usually involve decreased access to medication by the patients, and biases in pain assessment and management by healthcare providers; and differential workers compensation for pain-related claims (5). A meta-analysis utilizing data from 1989-2011 found that Hispanic and Black patients had a 22% and 30% lower rate of obtaining an opioid prescription compared to white patients, respectively (5). In 2010, due to better regulation of opioid prescriptions, heroin use and other synthetically produced opioids increased, leading to a crisis of opioid related deaths (6).
Opioid Use Disorder (OUD) is the chronic use of opioids that leads to habitual drug seeking and includes reduced self-control, participation in risky behavior and social impairments (7). Although treatment for OUD, discrimination continues to affect the care provided to the minority population (7). It is known that treatment for OUD can reduce the overdose rate, increase patient involvement in addiction programs when discharged and decrease overall health care utilization (8). Unfortunately, communities that have a higher number of Black and Hispanic residents have reduced health care resources that can provide the recommended interventions for OUD. When controlling for factors such as overdose burden, socioeconomic status and hospital risk factors; minority communities are still less likely to have access to essential harm reduction services(8).
FIGURE 1: U.S Drug Overdose death rate
[SEE ARTICLE from the CDC]
Analysis
Only 20% of patients with OUD get treatment despite the studied benefits such as reduced risk of mortality (10). Research has shown that racial minorities are less likely to obtain treatment for OUD from health care providers when compared to white counterparts(8). In 2019, Black and Hispanic with diagnosed OUD were 30% less likely than White patients to be offered treatment (11).
There have been numerous public strategies taken to improve opioid misuse. Unfortunately, public health campaigns primarily focus on White communities and ultimately decreased the rate of OUD and opioid related death for White patients alone rather than the combination with minority patients (12). As a result of minority patients receiving less community support and resources for OUD, individuals resort to self-medicating with fentanyl and heroin which increases opioid misuse within these populations (12). In 2019, opioid related mortality rates decreased by 0.3% in White patients but increased by 20% in Black patients (13).
A quantitative analysis on the intersection of race and opioid use disorder treatment observed how race influences treatment for OUD. This study used patient information from the Treatment Episode Data Set Discharges (TEDS-D), a nationwide study utilizing data of patients discharged from substance use disorder (SUD) treatment programs (14). The dataset includes information on treatment episodes and admissions to SUD treatment programs including programs in public and privately owned facilities. TEDS-D also included information from institutions such as state prisons. The study only used information from patients with a DSM-IV diagnosis of OUD between 2013 to 2017. From this data, researchers observed that being a minority is linked with a reduced chance of being referred to treatment by a healthcare worker. Data also showed that compared to their White counterparts, minority patients had a reduced likelihood of receiving appropriate OUD medication as part of the treatment plan. This study, as with many others, concluded that change is required to address this problem. This study primarily focused on policymakers and how to implement these findings to create interventions for OUD that acknowledge race. Public health interventions could help to address the discrepancies in treatment gaps that this study identified.
Discussion
Additional studies are needed to develop more efficacious strategies to address race for OUD. Across multiple studies, it is noted that areas with more economic instability and distress reported higher drug use. There are other factors discussed such as income, housing instability, transportation, insurance, biases, and mistrust in the healthcare system that influence access to treatment. Interventions in the local, state, and national policy levels are critical to tackle these issues.
Interventions such as linkage and retention in care while not criminalizing patients with OUD and access to treatment and harm reduction services are beneficial in minority communities. Ultimately, intervention and prevention strategies must include evidence based and culturally receptive tools that use social determinants of health to reduce biases surrounding treatment. These tools include culturally targeted campaigns and hiring community prevention liaisons or ambassadors to assist with decreasing mistrust and increasing accessibility to treatment and reduction services. Opioid misuse is preventable. Integrating efforts with an emphasis on childhood experiences that increase the risk for OUD, as well as applying trauma-informed care, is essential for improving minority communities that have been affected by years of discriminatory policies.
President-elect Donald Trump’s incoming administration could try to remove fluoride from drinking water, according to Robert F. Kennedy Jr.
Kennedy, who was tapped last week by Trump to lead the Department of Health and Human Services, called fluoride an “industrial waste” and linked it to cancer and other diseases and disorders while campaigning for Trump.
“On January 20, the Trump White House will advise all U.S. water systems to remove fluoride from public water. Fluoride is an industrial waste associated with arthritis, bone fractures, bone cancer, IQ loss, neurodevelopmental disorders, and thyroid disease,” Kennedy wrote Nov. 2 on X. Kennedy linked to a video from an attorney who recently successfully sued the Environmental Protection Agency to take additional measures to regulate fluoride in drinking water.
Kennedy, who has long advocated ending water fluoridation, persisted with his pledge following Trump’s election win. When asked before the election whether his administration would remove fluoride from drinking water, Trump said, “Well, I haven’t talked to him about it yet, but it sounds OK to me. You know it’s possible.”
Kennedy is an influential vaccine skeptic whose campaign of conspiracy theories earned PolitiFact’s 2023 “Lie of the Year.”
Recent studies, however, have shown possible links between fluoride and bone problems and children’s IQs, particularly when fluoride is above the U.S. recommended levels.
“There is evidence that fluoride exposure has been associated with the diseases [and] disorders that RFK listed, but with caveats,” said Ashley Malin, who is an assistant professor in the University of Florida’s Epidemiology Department and has studied fluoride’s effects in pregnant women.
Malin referred to studies showing that higher fluoride exposure, particularly during pregnancy, is associated with reduced child IQ, and that prenatal exposure also is linked to decreased intellectual functioning and executive function. For high exposure in pregnancy, the studies showed symptoms associated with other neurobehavioral issues, such as attention-deficit/hyperactivity disorder.
However, many of these studies took place in countries other than the U.S. and looked at fluoride in drinking water at sometimes twice the United States’ recommended level. Also, some of the other ailments that Kennedy listed, such as an association with bone cancer, have less robust evidence and need more study.
“Aside from fluoride’s impacts on neurodevelopment, I think that there is more that we don’t know about health effects of low-level fluoride exposure than what we do know, particularly for adult health outcomes,” Malin said.
Subscribe to California Healthline’s free Daily Edition.
David Bellinger, a Harvard Medical School neurology professor and professor in Harvard School of Public Health’s Environmental Health Department, said the risk-benefit calculation of added fluoride differs depending on whether typical fluoride exposure levels cause health problems, or if problems occur only when recommended levels are exceeded.
“In toxicology, ‘the dose makes the poison’ is a long-standing principle,” he said. “So a general statement that fluoride is associated with diseases X, Y, and Z is not very helpful unless the dose that might be responsible is specified.”
PolitiFact contacted Kennedy through his Children’s Health Defense organization but received no reply. The organization sued PolitiFact and Meta related to a 2020 fact check. That lawsuit was dismissed by a federal court. The dismissal was upheld on appeal, and the case is pending a possible appeal to the U.S. Supreme Court.
What Is Fluoride and What Are Its Benefits?
Fluorideis a mineral naturally occurring in soil, water, and some foods that helps prevent tooth decay and cavities. It strengthens tooth enamel that acid from bacteria, plaque, and sugar can wear away.
Water fluoridation has been happening in the U.S. since 1945.
The federal Public Health Service first recommended fluoridation of tap water in 1962, but the decision still lies with states and municipalities. Around 72% of the U.S. population, or about 209 million people, had access to fluoridated water in 2022, the CDC reported. Fluoride also has been added to oral care products such as toothpaste and mouth rinse.
In 2015, U.S. health officials lowered the recommended amount of fluoride in drinking water to 0.7 milligrams per liter, saying a higher level was less necessary given other sources of fluoride, and that the lowered amount would still help protect teeth without staining them.
Pediatric dentists note that applying fluoride with toothpaste and rinses is beneficial, but small amounts circulating in the body via water consumption helps younger children who still have their baby teeth, because it can benefit the developing permanent teeth.
The American Dental Association says studies have shown that fluoride in community water systems prevents at least 25% of tooth decay in children and adults and that “for more than 75 years, the best scientific evidence has consistently shown that fluoridation is safe and effective.”
The association says on its website: “It’s similar to fortifying other foods and beverages — for example, fortifying salt with iodine, milk with vitamin D, orange juice with calcium, and bread with folic acid.”
According to the CDC, health experts and scientists from the U.S. and other countries have so far “not found convincing scientific evidence linking community water fluoridation with any potential adverse health effect or systemic disorder such as an increased risk for cancer, Down syndrome, heart disease, osteoporosis and bone fracture, immune disorders, low intelligence, renal disorders, Alzheimer’s disease, or allergic reactions.”
The agency says risks of water fluoridation are limited to dental fluorosis, which can alter dental enamel and cause white flecks, spots, lines, or brown stains on the teeth when too much fluoride is consumed.
Do Studies Show Fluoride Posing Any Other Risks?
Some studies have said that excess fluoride exposure, often at higher levels than the recommended U.S. limit, can harm infants’ and young children’s developing brains and that higher levels of fluoride exposure during pregnancy were associated with declines in children’s IQs.
A study published in May that Malin led with University of Southern California and Indiana University researchers suggested that fluoride exposure during pregnancy was linked to an increased risk of childhood neurobehavioral problems and said more studies were “urgently needed to understand and mitigate the impacts in the entire U.S. population.”
Experts noted prenatal fluoride exposure is most strongly linked to children’s IQ loss, and said timing of fluoride consumption might need to be considered when making recommendations.
A federal review of dozens of studies published in August by the Department of Health and Human Services’ National Toxicology Program concluded that higher levels of fluoride exposure were linked to lower IQs in children. But the report was based primarily on studies in countries such as Canada, China, India, Iran, Mexico, and Pakistan and involved fluoride levels at or above 1.5 milligrams per liter, twice the recommended U.S. limit. The authors said more research is needed to understand whether lower exposure has any adverse effects.
In the report, researchers said they found no evidence that fluoride exposure adversely affected adult cognition.
Bellinger, of Harvard, pointed to the review as an example of how the amount of fluoride matters. He noted how researchers concluded that a very small percentage of people in the U.S. are exposed to levels that correlate with IQ loss.
“Second, the fact that there are now multiple pathways of exposure to fluoride besides fluoridated water (toothpaste and other dental products, etc.) makes it really difficult to attribute a particular adverse effect to the fluoride added to the water,” he wrote via email. “It is the cumulative exposure from all sources that contribute to any adverse health effects.”
In September, a federal judge ordered the Environmental Protection Agency to further regulate fluoride in drinking water because of the potential risk that higher levels could affect children’s intellectual development.
U.S. District Judge Edward Chen wrote that the court’s finding didn’t “conclude with certainty that fluoridated water is injurious to public health,” saying it’s unclear whether the amount of fluoride typically added to water is causing children’s IQs to drop. But he wrote that there was enough risk to warrant investigation and that the EPA must act to further regulate it. The ruling did not specify what actions the agency should take, and the EPA is reviewing the decision.
After the ruling, the American Association of Pediatrics issued a statement that fluoride in drinking water is safe for children and said the policy is based on a robust foundation of evidence.
Besides dental fluorosis, experts say that fluoride exposure over many years above the U.S. recommended amount can cause skeletal fluorosis, a rare condition that causes weaker bones, stiffness, and joint pain. Although the Public Health Service recommends a fluoride concentration of 0.7 milligrams per liter for community water systems, the EPA, under the Safe Drinking Water Act, sets enforceable standards for drinking-water quality. Currently, to prevent skeletal fluorosis, the EPA requires that water systems not exceed 4 milligrams of fluoride per liter of water.
Malin said she and her research team are investigating a potential link between fluoride and bone fractures. She said that although several studies have found high fluoride exposure associated with increased risk of bone fractures, and some have linked fluoride with thyroid disease, rigorous, U.S.-based studies haven’t been done.
The CDC concluded that recent research found no link between cancer risk and high levels of fluoride in drinking water.
The American Cancer Society reviewed a possible link between water fluoridation and cancer risk. An organization spokesperson pointed PolitiFact to its review and said it has no data showing a definitive answer.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
In March, newly installed Social Security chief Martin O’Malley criticized agency “injustices” that “shock our shared sense of equity and good conscience as Americans.”
He promised to overhaul the Social Security Administration’s often heavy-handed efforts to claw back money that millions of recipients — including people who are living in poverty, are elderly, or have disabilities — were allegedly overpaid, as described by a KFF Health News and Cox Media Group investigation last year.
“Innocent people can be badly hurt,” O’Malley said at the time.
Nearly eight months since he appeared before Congress and announced a series of policy changes, and with two months left in his term, O’Malley’s effort to fix the system has made inroads but remains a work in progress.
For instance, one change, moving away from withholding 100% of people’s monthly Social Security benefits to recover alleged overpayments, has been a major improvement, say advocates for beneficiaries.
“It is a tremendous change,” said Kate Lang of Justice in Aging, who called it “life-changing for many people.”
The number of people from whom the Social Security Administration was withholding full monthly benefits to recoup money declined sharply — from about 46,000 in January to about 7,000 in September, the agency said.
Asked to clarify whether those numbers and others provided for this article covered all programs administered by the agency, the SSA press office did not respond.
Another potentially significant change — relieving beneficiaries of having to prove that an overpayment was not their fault — has not been implemented. The agency said it is working on that.
Meanwhile, the agency seems to be looking to Congress to take the lead on a change some observers see as crucial: limiting how far back the government can reach to recover an alleged overpayment.
Barbara Hubbell of Watkins Glen, New York, called the absence of a statute of limitations “despicable.” Hubbell said her mother was held liable for $43,000 because of an SSA error going back 19 years.
“In what universe is that even legal?” Hubbell said. Paying down the overpayment balance left her mother “essentially penniless,” she added.
Subscribe to California Healthline’s free Daily Edition.
In response to questions for this article, Social Security spokesperson Mark Hinkle said legislation is “the best and fastest way” to set a time limit.
Establishing a statute of limitations was not among the policy changes O’Malley announced in his March congressional testimony. In an interview at the time, he said he expected an announcement on it “within the next couple few months.” It could probably be done by regulation, without an act of Congress, he said.
Speaking generally, Hinkle said the agency has “made substantial progress on overpayments,” reducing the hardship they cause, and “continues to work diligently” to update policies.
The agency is underfunded, he added, is at a near 50-year low in staffing, and could do better with more employees. The SSA did not respond to requests for an interview with O’Malley.
O’Malley announced the policy changes after KFF Health News and Cox Media Group jointly published and broadcast investigative reporting on the damage overpayments and clawbacks have done to millions of beneficiaries.
When O’Malley, a former Democratic governor of Maryland, presented his plans to three congressional committees in March, lawmakers greeted him with rare bipartisan praise. But the past several months have shown how hard it can be to turn around a federal bureaucracy that is massive, complex, deeply dysfunctional, and, as it says, understaffed.
Now O’Malley’s time may be running out.
Lang of Justice in Aging, among the advocacy groups that have been meeting with O’Malley and other Social Security officials, said she appreciates how much the commissioner has achieved in a short time. But she added that O’Malley has “not been interested in hearing about our feelings that things have fallen short.”
One long-standing policy O’Malley set out to change involves the burden of proof. When the Social Security Administration alleges someone has been overpaid and demands the money back, the burden is on the beneficiary to prove they were not at fault.
Cecilia Malone, 24, a beneficiary in Lithonia, Georgia, said she and her parents spent hundreds of hours trying to get errors corrected. “Why is the burden on us to ‘prove’ we weren’t overpaid?” Malone said.
It can be exceedingly difficult for beneficiaries to appeal a decision. The alleged overpayments, which can reach tens of thousands of dollars or more, often span years. And people struggling just to survive may have extra difficulty producing financial records from long ago.
What’s more, in letters demanding repayment, the government does not typically spell out its case against the beneficiary — making it hard to mount a defense.
Testifying before House and Senate committees in March, O’Malley promised to shift the burden of proof.
“That should be on the agency,” he said.
The agency expects to finalize “guidance” on the subject “in the coming months,” Hinkle said.
The agency points to reduced wait times and other improvements in a phone system known to leave beneficiaries on hold. “In September, we answered calls to our national 800 number in an average of 11 minutes — a tremendous improvement from 42 minutes one year ago,” Hinkle said.
Still, in response to a nonrepresentative survey by KFF Health News and Cox Media Group focused on overpayments, about half of respondents who said they contacted the agency by phone since April rated that experience as “poor,” and few rated it “good” or “excellent.”
The survey was sent to about 600 people who had contacted KFF Health News to share their overpayment stories since September 2023. Almost 200 people answered the survey in September and October of this year.
Most of those who said they contacted the agency by mail since April rated their experience as “poor.”
Jennifer Campbell, 60, a beneficiary in Nelsonville, Ohio, said in late October that she was still waiting for someone at the agency to follow up as described during a phone call in May.
“VERY POOR customer service!!!!!” Campbell wrote.
“Nearly impossible to get a hold of someone,” wrote Kathryn Duff of Colorado Springs, Colorado, who has been helping a disabled family member.
Letters from SSA have left Duff mystified. One was postmarked July 9, 2024, but dated more than two years earlier. Another, dated Aug. 18, 2024, said her family member was overpaid $31,635.80 in benefits from the Supplemental Security Income program, which provides money to people with little or no income or other resources who are disabled, blind, or at least 65. But Duff said her relative never received SSI benefits.
What’s more, for the dates in question, payments listed in the letter to back up the agency’s math didn’t come close to $31,635.80; they totaled about a quarter of that amount.
Regarding the 100% clawbacks, O’Malley in March said it’s “unconscionable that someone would find themselves facing homelessness or unable to pay bills, because Social Security withheld their entire payment for recovery of an overpayment.”
He said that, starting March 25, if a beneficiary doesn’t respond to a new overpayment notice, the agency would default to withholding 10%. The agency warned of “a short transition period.”
That change wasn’t automated until June 25, Hinkle said.
The number of people newly placed in full withholding plummeted from 6,771 in February to 51 in September, according to data the agency provided.
SSA said it would notify recipients they could request reduced withholding if it was already clawing back more than 10% of their monthly checks.
Nonetheless, dozens of beneficiaries or their family members told KFF Health News and Cox Media Group they hadn’t heard they could request reduced withholding. Among those who did ask, roughly half said their requests were approved.
According to the SSA, there has been almost a 20% decline in the number of people facing clawbacks of more than 10% but less than 100% of their monthly checks — from 141,316 as of March 8 to 114,950 as of Oct. 25, agency spokesperson Nicole Tiggemann said.
Meanwhile, the number of people from whom the agency was withholding exactly 10% soared more than fortyfold — from just over 5,000 to well over 200,000. And the number of beneficiaries having any benefits withheld to recover an overpayment increased from almost 600,000 to almost 785,000, according to data Tiggemann provided.
Lorraine Anne Davis says she hasn’t received her monthly Social Security payment since June due to an alleged overpayment. Her Medicare premium was being deducted from her monthly benefit, so she has been left to pay that out-of-pocket.(The Davis family)
Lorraine Anne Davis, 72, of Houston, said she hasn’t received her monthly Social Security payment since June due to an alleged overpayment. Her Medicare premium was being deducted from her monthly benefit, so she’s been left to pay that out-of-pocket.
Davis said she’s going to need a kidney transplant and had been trying to save money for when she’d be unable to work.
A letter from the SSA dated April 8, 2024, two weeks after the new 10% withholding policy was slated to take effect, said it had overpaid her $13,538 and demanded she pay it back within 30 days.
Apparently, the SSA hadn’t accounted for a pension Davis receives from overseas; Davis said she disclosed it when she filed for benefits.
In a letter to her dated June 29, the agency said that, under its new policy, it would change the withholding to only 10% if she asked.
Davis said she asked by phone repeatedly, and to no avail.
“Nobody seems to know what’s going on” and “no one seems to be able to help you,” Davis said. “You’re just held captive.”
In October, the agency said she’d receive a payment — in March 2025.
Marley Presiado, a research assistant on the Public Opinion and Survey Research team at KFF, contributed to this report.
Do you have an experience with Social Security overpayments you’d like to share? Click here to contact our reporting team.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
A California agency charged with slowing health costs has set a lofty goal for insurers to direct 15% of their spending to primary care by 2034, part of the state’s effort to expand the primary care workforce and give more people access to preventive care services.
The board of the state Office of Health Care Affordability in October set its benchmark well above the industry’s current 7% primary care spending rate, in hopes of improving Californians’ health and reducing the need for costlier care down the road.
“It’s ambitious but achievable,” said Elizabeth Landsberg, director of the state’s Department of Health Care Access and Information, which oversees the affordability agency. “Plans and health systems need time to build the infrastructure to really change the way they’re providing care.”
But California’s target comes just six months after the affordability board set an annual cap of 3.5% for overall growth in health care spending, potentially squeezing insurers from two sides.
“How these two policies will interact is unclear and we believe it is important to not lose sight of our overall goal of reducing the growth of health care costs,” Mary Ellen Grant, a spokesperson for the California Association of Health Plans, said in a statement.
The affordability agency argues health plans are best positioned to promote more spending on preventive care services, since insurers are the ones that negotiate payment with providers. Landsberg said health plans could dangle incentives, such as offering higher reimbursement rates for primary care providers or paying for comprehensive care instead of for individual visits.
If successful, the agency says, the spending target could expand the primary care workforce through the hiring of staff and lead to better health management, disease prevention, and early diagnosis and treatment for more patients across the state.
Subscribe to California Healthline’s free Daily Edition.
California faces a shortage of primary care providers, which has limited people’s access to preventive care. Approximately 6 million Californians live in parts of the state where there aren’t enough doctors to meet people’s needs, according to a data analysis by KFF, a health information nonprofit that includes KFF Health News, the publisher of California Healthline.
A 2021 report by the National Academies of Sciences, Engineering, and Medicine found that while more than 35% of health care visits in the U.S. are to primary care physicians, only about 5% of health spending is on primary care. That’s compared with about 13% for some other developed nations.
“People have high regard for primary care, understand how important it is,” said Kevin Grumbach, a professor of family and community medicine at the University of California-San Francisco who helped develop the state’s primary care target. “They way overestimate how much of their tax dollars are actually going to support primary care.”
Beginning next year, the affordability agency will start collecting data on how much health plans spend annually on primary care, particularly in settings such as community-based clinics, schools, and homeless shelters. Doctors, nurses, and pharmacists are among the providers whose services can be counted toward the goal. But the agency is excluding obstetricians, who sometimes serve as primary care providers for pregnant women, to focus on those offering “coordinated, comprehensive care” for patients.
Health plans will be expected to increase primary care spending from 0.5% to 1% of their total medical expenses each year until 15% is reached in 2034.
At least six states — Colorado, Connecticut, Delaware, Oregon, Rhode Island, and Washington — have already implemented primary care targets with some success. Rhode Island, which set a 10.7% goal, more than doubled its primary care spending from 2008 to 2018, while also reducing overall health spending.
The Biden administration has launched initiatives to improve primary care, but it has not set a primary care target for Medicare.
In California, the affordability agency collects health care spending data that captures nearly 33 million of the state’s 39 million residents. The agency said it will begin to collect primary care spending data in fall 2025, but that information may not be released for two more years.
The state agency lacks enforcement authority in primary care spending, so to get health plans to hit the target, the agency is dangling financial incentives. At a primary care summit at the University of California-Davis in October, Landsberg said the agency could allow insurers to exceed the 3.5% overall growth cap if they show their spending went to boost primary care.
Efrain Talamantes, chief operating officer for AltaMed Health Services, one of the state’s largest federally qualified community health centers, said these payments could help the health center expand services by training and hiring staff.
If health plans comply, the policy should lead to more primary care providers, timelier appointments, and better health outcomes, especially for disadvantaged communities that historically haven’t had good access to care, Talamantes said.
“We should see an improvement where people are able to access their primary care the same day,” he said.
As discussions continue, the state is working on targets to increase spending on behavioral health, another underinvested service. A vote on that measure could come next summer.
Robert F. Kennedy Jr., President-elect Donald Trump’s pick to lead the Department of Health and Human Services, is coming into the nomination process in an unusual position, with a long list of his own policy priorities separate from the president-elect’s, and a public promise by Trump to let him “go wild” on his ideas.
Céline Gounder, the editor-at-large for public health at KFF Health News and a CBS News medical contributor, answers questions below about the role Kennedy has been tapped to take on and some of the ideas in the sweeping “Make America Healthy Again” platform he may try to push through.
Q: What is the role of the Department of Health and Human Services, and how much power does the HHS secretary have over its work?
A: The U.S. Department of Health and Human Services comprises several agencies and offices including the National Institutes of Health, the Centers for Disease Control and Prevention, the Food and Drug Administration, the Centers for Medicare & Medicaid Services, the Office of the Surgeon General, and much more.
There is a big difference between political appointees and career civil servants. Political appointees set strategic priorities and align their department or agency’s policies with the current administration’s objectives. Civil servants have the institutional knowledge to know how to get things done and have specialized scientific or technical expertise. Scientific questions require specialized expertise. This is why there are career scientists who advise the HHS secretary, NIH director, CDC director, and FDA commissioner.
The HHS secretary has the authority to establish regulations that govern health, including food and drug safety, public health, and health care quality. The HHS secretary can declare public health emergencies and coordinate federal responses to health crises, such as disease outbreaks or natural disasters. The secretary wields significant influence over the department’s policies and its constituent agencies, which include the CDC, FDA, NIH, and others.
The HHS secretary is also in a position to shape public opinion if given a platform to do so by the media. Absent media attention, their influence on public opinion is more limited. We in the media have a responsibility to fact-check their statements and hold those in power accountable — regardless of who is in power.
Q: One of Kennedy’s most controversial stances is his criticism of vaccines, promoting the idea that they cause autism, among other conditions, and claiming “there’s no vaccine that is safe and effective.” What is the reality?
A: Extensive research has conclusively shown that vaccines do not cause autism. The “research” behind these claims was retracted due to ethical violations and sloppy work. The doctor who originally made those claims lost his medical license as a result of his professional misconduct.
For parents whose kids have autism or people who have autism, this matters. For too long, claims about the safety of vaccines have not only put people at unnecessary risk of getting illnesses that vaccines can prevent, but have also been a red herring, distracting people from the real causes of autism and how to diagnose them and treat them. That distraction is unproductive and harmful.
Secondly, nothing in this world is 100% safe and effective. It’s all about weighing risks, the pros and cons. Is one choice more beneficial or more risky? Do the pros of wearing a seat belt in the car outweigh the risks? Do the pros of exercising regularly outweigh the risks of not exercising? You could get injured while exercising. Do the pros of vaccinating instead of allowing infectious diseases to spread in the community outweigh the cons? Yes, yes, and yes.
Q: Kennedy has said he wants to leave it up to individuals to decide whether to vaccinate themselves or their children. What impact could that have?
A: Increasingly, people are formulating opinions about vaccines based not on science but on Google searches, social media, what family and friends think, and personal observation. That is not research. Research is formulating a hypothesis and trying to disprove that hypothesis. It means you understand how to differentiate correlation from causation. And it means doing repeated experiments to show consistency, not just a chance or random result.
This isn’t a question of whether people are smart or not. But most people don’t have the training, experience, and context to objectively assess the pros and cons of vaccination. You wouldn’t want me repairing your car’s transmission or brake system. I’m not stupid, but I have no training or experience in this.
The risk of leaving these decisions to untrained individuals is that these decisions won’t be made on science. They will be made based on emotion and confirmation bias, which is to say, Google searches looking for opinions that line up with your preexisting beliefs or inclinations. This will put kids at risk, and because vaccines protect against transmissible infectious diseases this will put others in the community at risk, especially other kids and people who are immunocompromised.
Q: Kennedy has also said chemicals in food are tied to autism as well as psychotic episodes and depression. What do we know about the connection between food and mental health?
A: He’s not wrong that there is a relationship between diet and autism as well as diet and mental health. These are areas of ongoing research. No diet has been proven to cure or universally improve autism or mental health symptoms, but certain dietary interventions improve symptoms in some people. These dietary changes may include elimination of ultraprocessed foods, eliminating gluten, and avoiding certain food additives or preservatives.
Q: Kennedy has said one of the Trump administration’s first acts will be to work to remove fluoride from drinking water, arguing it’s connected to cancer, IQ loss, thyroid disease, and other health problems. Why is fluoride in drinking water, and is it safe?
A: Fluoride is put in the water to reduce the risk of cavities, especially in kids.
As with many things, fluoride safety is all about dose. Drinking a few glasses of water a day is healthy. Drinking from a fire hydrant all day would land you in the hospital. The level of fluoride in U.S. water is safe and protects against tooth decay.
When municipalities stopped putting fluoride in the water, cavity rates went up. This was observed, for example, in Calgary, Canada, and in Juneau, Alaska.
There are parts of the world, including India, China, and East Africa, where fluoride levels 30 to 40 times higher than levels in the U.S. have been found to be harmful. But we don’t have anywhere near those levels of fluoride in our water.
But Kennedy’s statement demonstrates a common misunderstanding about public health authorities in the U.S. We are the United States of America — public health powers reside at the state level. The federal government has the authority to tax and spend and to regulate commerce across state lines, and federal government authorities derive from that.
The CDC provides scientific guidance to help state and local authorities to make informed decisions. The CDC does not mandate fluoridation. The EPA sets the maximum allowable fluoride concentration in public water systems. But states have the authority to mandate fluoridation or can leave it up to local jurisdictions.
Q: Kennedy has criticized multiple public health agencies he could now lead. He has said the FDA’s “war on public health is about to end,” claiming the agency suppresses anything that “advances human health and can’t be patented” by pharmaceutical companies. What do you make of these criticisms?
A: This again demonstrates a misunderstanding of federal agency authority. Congress has passed laws that give the FDA specific authority to regulate drugs, supplements, and food, and those laws grant the FDA different powers over drugs, supplements, and food.
If anything, given the Supreme Court’s “major questions doctrine,” the courts can determine that agencies may not make regulations on issues of significant economic or political importance unless Congress has clearly authorized such actions. For example, in the case FDA v. Brown & Williamson Tobacco Corp. (2000), the Supreme Court concluded that the FDA lacked the power to regulate tobacco. In 2009, Congress passed the Family Smoking Prevention and Tobacco Control Act, granting the FDA the authority to regulate tobacco.
Drugs require FDA approval before they can be marketed. Under the law, drugs are defined as substances used to diagnose, treat, or prevent disease.
Supplements don’t need FDA approval before they are sold. The FDA monitors dietary supplements once they are on the market and can take action if they are unsafe or if they make claims about diagnosis, treatment, or prevention of disease.
Dietary supplement manufacturers often choose not to seek FDA approval to market their products as drugs because:
There are less stringent requirements on dietary supplements than on drugs.
The FDA approval process is expensive and lengthy. Clinical trials take years to conduct and cost millions of dollars. Manufacturers foot the bill for clinical trials.
Dietary supplements can be sold directly to consumers without a prescription.
The manufacturer decides whether it wants to seek FDA approval for a drug or if it wants to market a product as a dietary supplement — and that decision typically comes down to time and money. Pharmaceutical companies are less inclined to invest millions of dollars in clinical trials of unpatented treatments due to the lack of exclusive marketing rights (in other words, a time-limited monopoly), which can affect profitability.
The FDA often goes after supplement brands that test this line when it sees companies marketing products with claims that amount to what should be regulated as a drug. This is why supplements often carry a disclaimer that they aren’t being sold to “diagnose, treat, cure, or prevent any disease.” Kennedy has praised the supplement industry for “fighting back,” following a court action over an anti-aging supplement that the FDA argued should be regulated as a drug.
Finally, the FDA doesn’t grant patents. That’s the job of the U.S. Patent and Trademark Office.
Q: Trump has said Kennedy will “end the Chronic Disease epidemic.” What are some of the positive actions he could take if he becomes HHS secretary to reduce chronic disease in the U.S.?
A: Kennedy has called for greater regulation of food additives and ultraprocessed foods. Ultraprocessed foods in American diets have led to an explosion in obesity, diabetes, high blood pressure, and other chronic disease.
However, it’s unclear which factions within Trump’s orbit will prevail. Congress may have to give the FDA the authority to regulate more aggressively and the funding to enforce those regulations. Historically, the Republican Party has been opposed to regulation. Trump’s chief of staff pick, Susie Wiles, is a longtime lobbyist who has worked on behalf of the food, insurance, and tobacco industries.
The Heritage Foundation’s Project 2025 — which involved a number of former Trump advisers, but which Trump has tried to distance himself from — would roll back dietary guidelines, making it harder to fight ultraprocessed foods.
En abril, cuando apenas llevaba 12 semanas de embarazo, Kathleen Clark estaba en la recepción de su ginecólogo-obstetra cuando le pidieron que pagara $960, el total que la consulta calculaba que tendría que pagar después del parto.
Clark, de 39 años, se sorprendió de que le pidieran pagar esa cantidad en su segunda visita prenatal. Normalmente, las pacientes reciben la factura después que el seguro haya pagado su parte, y en el caso de las embarazadas eso suele ocurrir cuando termina el embarazo. Pasarían meses antes de que la consulta presentara el reclamo a su seguro médico.
Clark dijo que se sintió atrapada. La consulta de obstetricia de Cleveland, Tennessee, estaba asociada a un centro de maternidad donde ella quería dar a luz. Además, ella y su marido llevaban mucho tiempo deseando tener un hijo. Y Clark se sentía especialmente sensible porque unas semanas antes había muerto su madre.
“Estás ahí, en la ventanilla, rodeada de gente, y tratas de ser lo más amable posible”, recordó Clark, entre lágrimas. “Así que lo pagué”.
En las comunidades sobre bebés en internet y en otros foros de las redes sociales, las embarazadas afirman que sus proveedores les piden que paguen antes de lo previsto. La práctica es legal, pero los defensores de los pacientes la califican de poco ética. Los médicos alegan que pedir el pago por adelantado les garantiza una compensación por sus servicios.
Es difícil saber con qué frecuencia ocurre porque se considera una transacción privada entre el proveedor y el paciente. Por lo tanto, los pagos no se registran en los datos de reclamos de seguros y, por ende, los expertos no los analizan.
Pacientes, expertos en facturación médica y activistas afirman que esta práctica de facturación provoca una ansiedad inesperada en un momento de estrés y presión financiera ya de por sí elevados. En ocasiones, las estimaciones pueden ser superiores a lo que el paciente deba en última instancia y obligan a las personas a luchar por un reembolso si la cantidad abonada era superior a la factura final.
Los pagos por adelantado también ponen trabas a las mujeres que quieran cambiar de proveedor si no están satisfechas con la atención. En algunos casos, pueden hacer que las mujeres renuncien por completo a la atención prenatal, sobre todo en lugares donde existen pocas opciones de atención materna.
Expertos en facturación médica y salud de la mujer creen que las consultas de ginecología y obstetricia adoptaron esta práctica para gestionar el elevado costo de la atención materna y la forma en que se factura en Estados Unidos.
Cuando un embarazo llega a término, los ginecólogos y obstetras suelen presentar un único reclamo al seguro por los cuidados prenatales rutinarios, el trabajo de parto, el parto y, a menudo, la atención posparto. Esta práctica de agrupar toda la atención materna en un único código de facturación comenzó hace tres décadas, según Lisa Satterfield, directora de salud y política de pagos del American College of Obstetricians and Gynecologists. Sin embargo, la facturación agrupada ha quedado obsoleta.
Antes, las pacientes embarazadas estaban sujetas a copagos por cada visita prenatal, lo que podía llevarlas a saltarse citas cruciales para ahorrar dinero. Pero ahora la Ley de Cuidado de Salud a Bajo Precio (ACA) exige que todas las aseguradoras comerciales cubran íntegramente determinados servicios prenatales. Además, cada vez es más frecuente que las embarazadas cambien de proveedor o que diferentes proveedores se encarguen de la atención prenatal y el parto, sobre todo en las zonas rurales, donde son frecuentes los traslados de pacientes.
Algunos proveedores afirman que los pagos por adelantado les permiten repartir los pagos únicos a lo largo del embarazo para asegurarse de que se los compensa por la atención que prestan, aunque finalmente no atiendan el parto.
“Desgraciadamente hay personas que no cobran por su trabajo”, afirmó Pamela Boatner, partera en un hospital de Georgia.
Aunque cree que las mujeres deben recibir atención durante el embarazo independientemente de su capacidad de pago, también entiende que algunos proveedores quieran asegurarse de que no se ignora su factura después de que nazca el bebé. Los nuevos padres pueden verse desbordados por las facturas del hospital y los costos de cuidar a un nuevo hijo, y pueden no tener ingresos suficientes si uno de los progenitores no trabaja, explicó Boatner.
En Estados Unidos, tener un bebé puede resultar caro. Las personas que están cubiertas por un seguro médico a través de grandes empresas pagan un promedio de unos $3.000 de su bolsillo por los cuidados durante el embarazo, el parto y el posparto, según el Peterson-KFF Health System Tracker. Además, muchos optan por planes médicos con deducibles elevados, lo que les obliga a asumir una mayor parte de los costos. De los 100 millones de estadounidenses con deudas médicas, el 12% atribuye al menos parte de ellas a los cuidados de maternidad, según una encuesta de KFF de 2022.
Las familias necesitan tiempo para ahorrar y poder así hacer frente a los elevados costos del embarazo, el parto y el cuidado de los hijos, en especial si no tienen licencia por maternidad remunerada, dijo Joy Burkhard, CEO del Policy Center for Maternal Mental Health, un think tank con sede en Los Angeles. Pedirles que paguen por adelantado “es un golpe bajo”, agregó. “¿Y si no tienes dinero? ¿Lo cargas a tarjetas de crédito y esperas que funcione?”.
Calcular los costos finales del parto depende de múltiples factores, como el momento del embarazo, las prestaciones del plan y las complicaciones de salud, afirmó Erin Duffy, investigadora de políticas de salud del Centro Schaeffer de Política y Economía de la Salud de la Universidad del Sur de California. La factura final para la paciente no está clara hasta que el plan de salud decide qué parte cubrirá, explicó.
Pero a veces se elimina la opción de esperar a la aseguradora.
Durante el primer embarazo de Jamie Daw, en 2020, su ginecólogo-obstetra aceptó su negativa a pagar por adelantado porque Daw quería ver la factura final. Pero en 2023, durante su segundo embarazo, en una consulta privada de obstetricia de Nueva York le dijeron que, como tenía un plan con deducible alto, era obligatorio pagar $2.000, en pagos mensuales.
Daw, investigadora de políticas de salud en la Universidad de Columbia, dio a luz en septiembre de 2023 y recibió un cheque de reembolso ese noviembre por $640 para cubrir la diferencia entre la estimación y la factura final.
“Yo me dedico a estudiar los seguros de salud”, dijo. “Pero una no se imagina lo enormemente complicado que es cuando lo vives en persona”.
Aunque ACA obliga a las aseguradoras a cubrir algunos servicios prenatales, no prohíbe a los proveedores enviar la factura final a los pacientes antes de tiempo. Sería un reto político y práctico para los gobiernos estatales y federal intentar regular el momento de la solicitud de pago, señaló Sabrina Corlette, codirectora del Centro de Reformas de Seguros de Salud de la Universidad de Georgetown. Los grupos de presión médicos son poderosos y los contratos entre aseguradoras y proveedores médicos están protegidos por derechos de propiedad intelectual.
Debido a la zona gris legal, Lacy Marshall, corredora de seguros de Rapha Health and Life en Texas, aconseja a sus clientes que pregunten a la aseguradora si pueden negarse a pagar por adelantado su deducible. Algunos planes prohíben a los proveedores de su red exigir el pago por adelantado.
Si la aseguradora les dice que pueden negarse a pagar por adelantado, Marshall les recomienda a los clientes establecer una relación con una consulta antes de negarse a pagar, de modo que el proveedor no pueda rechazar el tratamiento.
Clark dijo que alcanzó el deducible de su seguro después de pagar las pruebas genéticas, las ecografías adicionales y otros servicios con su cuenta de salud de gastos flexibles. Entonces llamó a la consulta de su ginecólogo y pidió que le devolvieran el dinero.
“Perdí el miedo”, dijo Clark, que antes había trabajado en una aseguradora de salud y en un consultorio médico. Recibió un primer cheque por la mitad de los $960 que había pagado inicialmente.
En agosto, Clark fue trasladada al hospital después que su presión arterial se disparara. Un especialista en embarazos de alto riesgo, y no su ginecólogo-obstetra original, atendió el parto prematuro de su hijo Peter mediante cesárea de urgencia a las 30 semanas de embarazo.
Hasta que no resolvió la mayoría de las facturas del parto no recibió el resto del reembolso de la otra consulta de ginecología y obstetricia.
El último cheque llegó en octubre, pocos días después de que Clark saliera del hospital con Peter para llevarlo a su hogar y tras múltiples llamadas a la consulta. Dijo que todo eso sumó estrés a un período ya de por sí estresante.
“¿Por qué tengo que pagar el precio como paciente?”, se preguntó. “Sólo intento tener un bebé”.
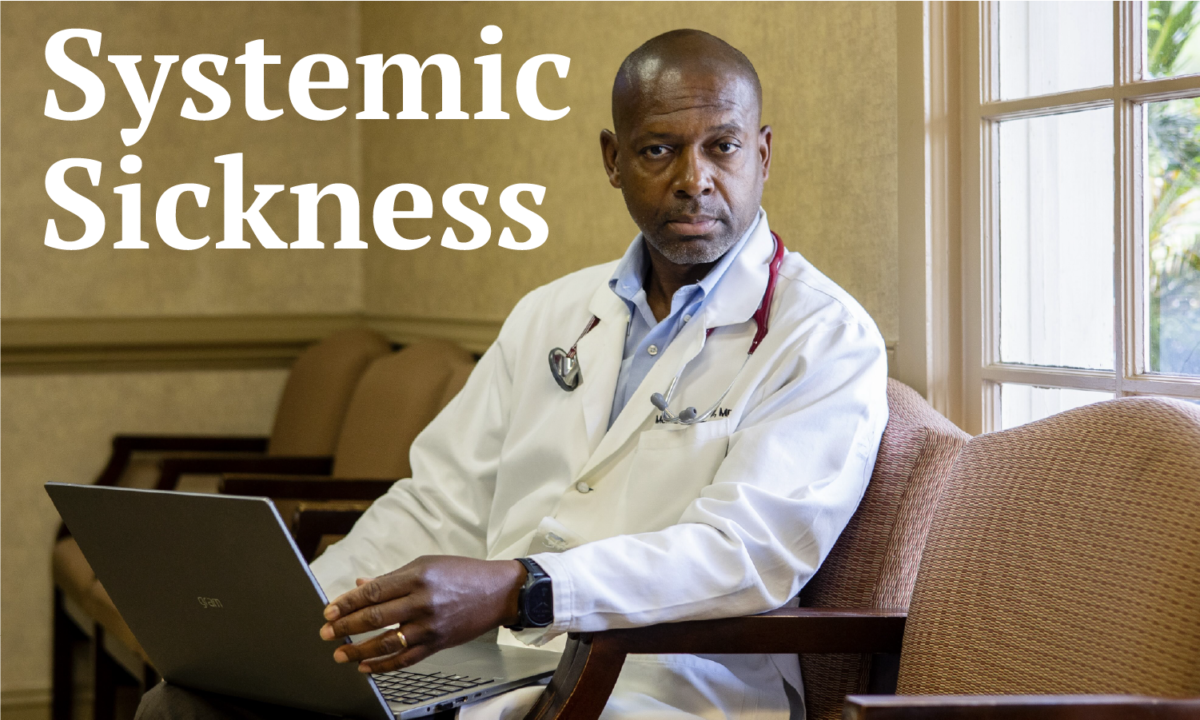
The United States has made almost no progress in closing racial health disparities despite promises, research shows. The government, some critics argue, is often the underlying culprit.
KFF Health News undertook a yearlong examination of how government decisions undermine Black health — reviewing court and inspection records and government reports, and interviewing dozens of academic researchers, doctors, politicians, community leaders, grieving moms, and patients.
During the past two decades there have been 1.63 million excess deaths among Black Americans relative to white Americans. That represents a loss of more than 80 million years of life, according to a 2023 JAMA study.
The video features senior correspondents Fred Clasen-Kelly and Renuka Rayasam, along with Morris Brown, a family care physician in Kingstree, South Carolina.
Learn more about the “Systemic Sickness” series here.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.