Raymond Llano carries a plastic bag with everything he owns in one hand, a cup of coffee in the other, and the flattened cardboard box he uses as a bed under his arm as he waits in line for lunch at Glide Memorial Church in San Francisco. At 55, he hasn’t had a home for 15 years, since he lost a job at Target.
Llano once tried to get on public assistance but couldn’t — something, he said, looking perplexed, about owing the state money — and he’d like to apply again.
But beginning next year, if he does, he’ll face a new city requirement that single adults with no dependents who receive cash benefits be screened for illegal drug use and, if deemed necessary, enter treatment. San Francisco’s voters approved the new mandate in March.
Llano has no objection to being screened. He said he uses cannabis, which is legal in California, though not federally, but does not use other drugs. Nonetheless, he said, “I suppose I would try recovery.”
Another man in the free-lunch line, Francis Farrell, 56, was far less agreeable. “You can screen me,” he said, raising his voice, “but I don’t think you should force me into your idea of treatment.”
No one will be forced to undergo substance abuse treatment, nor will anyone be subject to drug testing, San Francisco officials insist. Rather, starting in January 2025, San Francisco’s public assistance recipients who screen positive for addiction on a 10-question drug abuse test will be referred to treatment. Those who refuse or fail to show up for treatment will forfeit the $109 a month that the city grants to homeless adults who qualify for city shelters or supportive housing, or the $712 a month it grants to adults with home addresses.
The city famous for its tolerance is resorting to tough love.
Subscribe to California Healthline’s free Daily Edition.
Trent Rhorer, executive director of the San Francisco Human Services Agency, cited three reasons for the new measure, which was fashioned after similar policies in Los Angeles and New York: to incentivize people with a substance use disorder to enter treatment, to prevent taxpayer money from being used to buy illegal drugs, and to dissuade drug seekers from moving to San Francisco.
“We’re giving them the opportunity to engage in something, without requiring sobriety, to hopefully get on a path to recovery,” Rhorer told California Healthline.
When Mayor London Breed introduced the ballot initiative known as Measure F in a news conference last year, she called it an incentive to encourage drug-addicted recipients of public assistance to enter “into a program that will help save their life.” Accidental overdoses killed more than 800 people in San Francisco last year.
But in the eyes of many health care providers, researchers, and harm reduction advocates, the measure is neither an incentive nor an opportunity.
The policy was designed to have “a coercive, punitive effect” and could do more harm than good, said Vitka Eisen, president and chief executive of HealthRIGHT 360, San Francisco’s largest drug treatment provider.
“It would have been an interesting project, much more in the spirit of San Francisco as a hub of innovation, to figure out if we can identify people with substance use disorder. And if they go into treatment and stay for a period of time, they’ll get an increased benefit,” Eisen said.
About 5,800 people in the city currently receive benefits from the County Adult Assistance Programs, or CAAP. Under Measure F, those who acknowledge drug abuse on the screening test but refuse treatment and live in city-provided shelter will lose their cash benefits but can maintain their shelter, Rhorer said. However, CAAP recipients who refuse treatment and depend on public assistance to pay their rent in private housing could lose their homes.
The city will give recipients three chances to show up for treatment and will pay rent directly to a landlord for one month, Rhorer said. Measure F came in response to the grim conditions on some San Francisco streets, where men and women lie on sidewalks, often blocking passersby with their arms and legs splayed, or stand bent over, frozen like statues. Many use fentanyl, a synthetic opioid that has turned a long-standing homelessness problem into a public health emergency.
Paul Harkin, from the nonprofit Glide, hands out Narcan, fentanyl detection packets, and tinfoil in an alleyway in San Francisco on Feb. 3, 2020. (Nick Otto for the Washington Post via Getty Images)
Many homeless people in San Francisco use fentanyl, a synthetic opioid that has turned a long-standing homelessness problem into a public health emergency. (Jessica Christian/San Francisco Chronicle via Getty Images)
About 12% of people who fatally overdosed in San Francisco last year were CAAP recipients, Rhorer said.
Compassion fatigue seems to have settled over this city known for its kindheartedness. Measure F proponents raised $667,000 — more than 17 times as much as opponents — largely from business executives and tech investors, according to the San Francisco Ethics Commission. Then in March, 58% of voters approved the measure.
Since fentanyl began replacing heroin around 2019, Rhorer said, “drug tourists” have flocked to San Francisco, where the opioid has been cheap and plentiful. Lenient law enforcement and relatively generous cash public assistance grants also have drawn people with addiction, he said, although police activity has increased since last spring.
A recent city report found that only 53% of the 718 people whom police cited for substance use over a 10-month period that ended in February said they lived in the city.
“People who live in San Francisco, who really need the most help, don’t get the help they need due to the influx of people coming from somewhere else,” said Cedric Akbar, who runs recovery programs and co-founded Positive Directions Equals Changes. “And should our tax dollars go to the ones in San Francisco, or are we going to take care of the whole country?”
Akbar began using heroin when he moved to San Francisco from Houston in the 1980s and has been in recovery for 31 years. He said he would have preferred even stricter requirements for eligibility for public assistance than those in Measure F but hopes the new mandate will at least help give people access to treatment.
The city’s capacity for treatment is also a concern. Eisen and others describe a dire shortage of behavioral health workers to staff treatment facilities and residential step-down units, which are crucial for housing those in recovery from drug addiction.
New programs funded by the recently approved Proposition 1 in California, which authorizes the state to spend $6.38 billion to build mental health treatment facilities and provide housing for homeless people, are meant to address the shortages.
Leslie Suen, an addiction medicine physician and an assistant professor at the University of California-San Francisco, fears that pushing CAAP recipients into treatment could turn them off. When people “were stigmatized, or coerced, or told they would face consequences if they didn’t do a certain thing,” she said, “that pushed them away from the health system even further.”
Though evidence suggests compulsory treatment can provide short-term benefits, it also can lead to long-term harm, the National Institute on Drug Abuse said in an email.
“To achieve the best outcomes,” the email said, treatment should be “delivered without stigma or penalty.”
Almost everyone with a substance use disorder enters treatment under some kind of pressure, whether from a parent, a spouse, an employer, or the criminal justice system, said Keith Humphreys, a Stanford University psychiatry professor.
Nonetheless, he questioned the morality of requiring welfare recipients, as opposed to criminals, to get drug treatment.
“I would never start with people who are poor but not committing crimes,” he said. “I would start with people who are harming others.”
A new analysis finds that graduating medical students were less likely to apply this year for residency training in states that ban or restrict abortion. That was true not only for aspiring OB-GYNs and others who regularly treat pregnant patients, but for all specialties.
Meanwhile, another study has found that more than 4 million children have been terminated from Medicaid or the Children’s Health Insurance Program since the federal government ended a covid-related provision barring such disenrollments. The study estimates about three-quarters of those children were still eligible and were kicked off for procedural reasons.
This week’s panelists are Julie Rovner of KFF Health News, Lauren Weber of The Washington Post, Joanne Kenen of the Johns Hopkins University schools of nursing and public health and Politico Magazine, and Anna Edney of Bloomberg News.
Among the takeaways from this week’s episode:
More medical students are avoiding applying to residency programs in states with abortion restrictions. That could worsen access problems in areas that already don’t have enough doctors and other health providers in their communities.
New threats to abortion care in the United States include not only state laws penalizing abortion pill possession and abortion travel, but also online misinformation campaigns — which are trying to discourage people from supporting abortion ballot measures by telling them lies about how their information might be used.
The latest news is out on the fate of Medicare, and a pretty robust economy appears to have bought the program’s trust fund another five years. Still, its overall health depends on a long-term solution — and a long-term solution depends on Congress.
In Medicaid expansion news, Mississippi lawmakers’ latest attempt to expand the program was unsuccessful, and a report shows two other nonexpansion states — Texas and Florida — account for about 40% of the 4 million kids who were dropped from Medicaid and CHIP last year. By not expanding Medicaid, holdout states say no to billions of federal dollars that could be used to cover health care for low-income residents.
Finally, the bankruptcy of the hospital chain Steward Health Care tells a striking story of what happens when private equity invests in health care.
Also this week, Rovner interviews KFF Health News’ Katheryn Houghton, who reported and wrote the latest KFF Health News-NPR “Bill of the Month” feature, about a patient who went outside his insurance network for a surgery and thought he had covered all his bases. It turned out he hadn’t. If you have an outrageous or incomprehensible medical bill you’d like to share with us, you can do that here.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
Newswise — A defining development of the 20th century that changed the course of public health was when governments around the world improved access to safe water, sanitation and hygiene. However, a binational study led by University of California San Diego researchers found that, during the peak of the COVID-19 pandemic, people experiencing homelessness and individuals who inject drugs in San Diego and the bordering city of Tijuana, Mexico often did not have access to these basic resources.
There are estimated to be 10,000 people who inject drugs in Tijuana and another 21,800 in San Diego, many of whom are experiencing homelessness.
Reporting in the International Journal for Equity in Health, study first author Alhelí Calderón Villarreal, M.D., M.P.H., who conducted the research as part of her doctoral dissertation as a student in the UC San Diego-San Diego State University Joint Doctoral Program in Public Health, wrote that access to water, sanitation and hygiene was very low by international standards, and lower than the national averages in the United States and Mexico, for people who inject drugs and live in San Diego and Tijuana.
“We found that even in Southern California — one of the wealthiest parts of the world — people who use drugs often go without access to water, showers and toilets. The lack of these basic services also places people who use drugs at risk of serious, but preventable, illnesses, and poses risks to society at large,” said Calderón Villarreal, who will graduate in June with a Doctor of Philosophy in Public Health from the Herbert Wertheim School of Public Health and Human Longevity Science at UC San Diego.
Researchers interviewed 586 people in Tijuana (202) and San Diego (384) between 2020 and 2021, when COVID-19 infection was highest and when having access to water, showers and toilets should have been a public health priority.
Researchers found that 78 percent of individuals interviewed did not have access to an acceptable toilet, 54 percent did not have regular access to showers, and 11 percent reported having insufficient access to drinking water. Only 38 percent of study participants had access to water and soap for handwashing and the same number of participants reported defecating outdoors, placing themselves and the general public at health risk.
Abscesses and vascular damage are common injuries among people who inject drugs. Unsafe water used for preparing drugs or cleaning wounds can lead to life-threatening health problems including the risk of viral, parasitic and bacterial infections which include multi-drug resistant organisms, said the study authors.
Twenty percent of study participants said they felt thirsty daily, without access to drinking water. In fact, nearly all participants – 96.9 percent – drank less water daily than is medically recommended for proper hydration.
“Access to water, sanitation and hygiene are needed in both cities to reduce disparities and improve health and well-being among people who inject drugs, especially for those who are unhoused. It also benefits public health for the region as a whole,” said senior author Georgia Kayser, Ph.D., assistant professor at the Herbert Wertheim School of Public Health.
Experiencing homelessness increased the difficulty of finding toilets, bathing facilities and clean water sources. This was made even more difficult if the individual was unsheltered or on the street. Compared to participants who had housing, those who were unsheltered were 3.1 times more likely to be unable to access clean water sources for cleansing wounds and abscesses and 2.6 for preparing drugs for injection. They were twice as likely to be unable to access basic drinking water, 1.8 times more unlikely to have bathing opportunities, and 1.7 times less likely to have access to sanitation.
Participants residing in Tijuana reported a lack of access to basic drinking water and body and hand hygiene significantly more often than those living in San Diego. In Tijuana, 30 percent of people had access to basic hygiene (handwashing with water and soap) and 37 percent to bathing compared to 47 percent and 50 percent respectively in San Diego.
While San Diego provides more public access to water, sanitation and hygiene services, both cities have similar challenges and therefore can implement similar solutions.
The study authors suggest two solutions. Ideally, provide safe and secure places to live with access to safe water and sanitation to improve overall health and wellbeing. In the interim, expand access to mobile hygiene services and public restrooms, for those who do not have a traditional housing setting. This could involve extending hours of operation for existing public facilities, creating more public restrooms, increasing the number of mobile water, sanitation and hygiene service providers, and the integration of showers and toilet facilities in harm reduction programs.
“Providing everyone with access to drinking water, sanitation and hygiene services is necessary to prevent disease transmission and improve public health in the region,” said Gudelia Rangel, Ph.D., professor and investigator at the Colegio de la Frontera Norte and Border Health Coalition, Baja California, Mexico.
Co-authors include: Lourdes Johanna Avelar Portillo, UC San Francisco; Daniela Abramovitz, UC San Diego; Shira Goldenberg, Shawn Flanigan, Penelope J. E. Quintana, all of San Diego State University; Alicia Harvey‑Vera, UC San Diego and Universidad de Xochicalco; Carlos F. Vera, UC San Diego; and Steffanie Strathdee, principal investigator, UC San Diego School of Medicine.
This research was funded, in part, by the National Institute of Drug Abuse (R01DA049644, 3R01DA04964403S2), National Council of Science and Technology (CONACYT) 2020 in Mexico, Fogarty International Center of the National Institutes of Health (D43TW009343), and the National Institute of Environmental Health Sciences (K01ES031697).
Disclosures: The authors report no conflicts of interest.
Isabella Rosario Blum was wrapping up medical school and considering residency programs to become a family practice physician when she got some frank advice: If she wanted to be trained to provide abortions, she shouldn’t stay in Arizona.
Blum turned to programs mostly in states where abortion access — and, by extension, abortion training — is likely to remain protected, like California, Colorado, and New Mexico. Arizona has enacted a law banning most abortions after 15 weeks.
“I would really like to have all the training possible,” she said, “so of course that would have still been a limitation.”
In June, she will start her residency at Swedish Cherry Hill hospital in Seattle.
According to new statistics from the Association of American Medical Colleges, for the second year in a row, students graduating from U.S. medical schools were less likely to apply this year for residency positions in states with abortion bans and other significant abortion restrictions.
Since the Supreme Court in 2022 overturned the constitutional right to an abortion, state fights over abortion access have created plenty of uncertainty for pregnant patients and their doctors. But that uncertainty has also bled into the world of medical education, forcing some new doctors to factor state abortion laws into their decisions about where to begin their careers.
Fourteen states, primarily in the Midwest and South, have banned nearly all abortions. The new analysis by the AAMC — a preliminary copy of which was exclusively reviewed by California Healthline before its public release — found that the number of applicants to residency programs in states with near-total abortion bans declined by 4.2%, compared with a 0.6% drop in states where abortion remains legal.
Notably, the AAMC’s findings illuminate the broader problems abortion bans can create for a state’s medical community, particularly in an era of provider shortages: The organization tracked a larger decrease in interest in residencies in states with abortion restrictions not only among those in specialties most likely to treat pregnant patients, like OB-GYNs and emergency room doctors, but also among aspiring doctors in other specialties.
Subscribe to California Healthline’s free Daily Edition.
“It should be concerning for states with severe restrictions on reproductive rights that so many new physicians — across specialties — are choosing to apply to other states for training instead,” wrote Atul Grover, executive director of the AAMC’s Research and Action Institute.
The AAMC analysis found the number of applicants to OB-GYN residency programs in abortion ban states dropped by 6.7%, compared with a 0.4% increase in states where abortion remains legal. For internal medicine, the drop observed in abortion ban states was over five times as much as in states where abortion is legal.
In its analysis, the AAMC said an ongoing decline in interest in ban states among new doctors ultimately “may negatively affect access to care in those states.”
Jack Resneck Jr., immediate past president of the American Medical Association, said the data demonstrates yet another consequence of the post-Roe v. Wade era.
The AAMC analysis notes that even in states with abortion bans, residency programs are filling their positions — mostly because there are more graduating medical students in the U.S. and abroad than there are residency slots.
Still, Resneck said, “we’re extraordinarily worried.” For example, physicians without adequate abortion training may not be able to manage miscarriages, ectopic pregnancies, or potential complications such as infection or hemorrhaging that could stem from pregnancy loss.
Those who work with students and residents say their observations support the AAMC’s findings. “People don’t want to go to a place where evidence-based practice and human rights in general are curtailed,” said Beverly Gray, an associate professor of obstetrics and gynecology at Duke University School of Medicine.
Abortion in North Carolina is banned in nearly all cases after 12 weeks. Women who experience unexpected complications or discover their baby has potentially fatal birth defects later in pregnancy may not be able to receive care there.
Gray said she worries that even though Duke is a highly sought training destination for medical residents, the abortion ban “impacts whether we have the best and brightest coming to North Carolina.”
Rohini Kousalya Siva will start her obstetrics and gynecology residency at MedStar Washington Hospital Center in Washington, D.C., this year. She said she did not consider programs in states that have banned or severely restricted abortion, applying instead to programs in Maryland, New Hampshire, New York, and Washington, D.C.
“We’re physicians,” said Kousalya Siva, who attended medical school in Virginia and was previously president of the American Medical Student Association. “We’re supposed to be giving the best evidence-based care to our patients, and we can’t do that if we haven’t been given abortion training.”
Another consideration: Most graduating medical students are in their 20s, “the age when people are starting to think about putting down roots and starting families,” said Gray, who added that she is noticing many more students ask about politics during their residency interviews.
And because most young doctors make their careers in the state where they do their residencies, “people don’t feel safe potentially having their own pregnancies living in those states” with severe restrictions, said Debra Stulberg, chair of the Department of Family Medicine at the University of Chicago.
Stulberg and others worry that this self-selection away from states with abortion restrictions will exacerbate the shortages of physicians in rural and underserved areas.
“The geographic misalignment between where the needs are and where people are choosing to go is really problematic,” she said. “We don’t need people further concentrating in urban areas where there’s already good access.”
After attending medical school in Tennessee, which has adopted one of the most sweeping abortion bans in the nation, Hannah Light-Olson will start her OB-GYN residency at the University of California-San Francisco this summer.
It was not an easy decision, she said. “I feel some guilt and sadness leaving a situation where I feel like I could be of some help,” she said. “I feel deeply indebted to the program that trained me, and to the patients of Tennessee.”
Light-Olson said some of her fellow students applied to programs in abortion ban states “because they think we need pro-choice providers in restrictive states now more than ever.” In fact, she said, she also applied to programs in ban states when she was confident the program had a way to provide abortion training.
“I felt like there was no perfect, 100% guarantee; we’ve seen how fast things can change,” she said. “I don’t feel particularly confident that California and New York aren’t going to be under threat, too.”
As a condition of a scholarship she received for medical school, Blum said, she will have to return to Arizona to practice, and it is unclear what abortion access will look like then. But she is worried about long-term impacts.
“Residents, if they can’t get the training in the state, then they’re probably less likely to settle down and work in the state as well,” she said.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
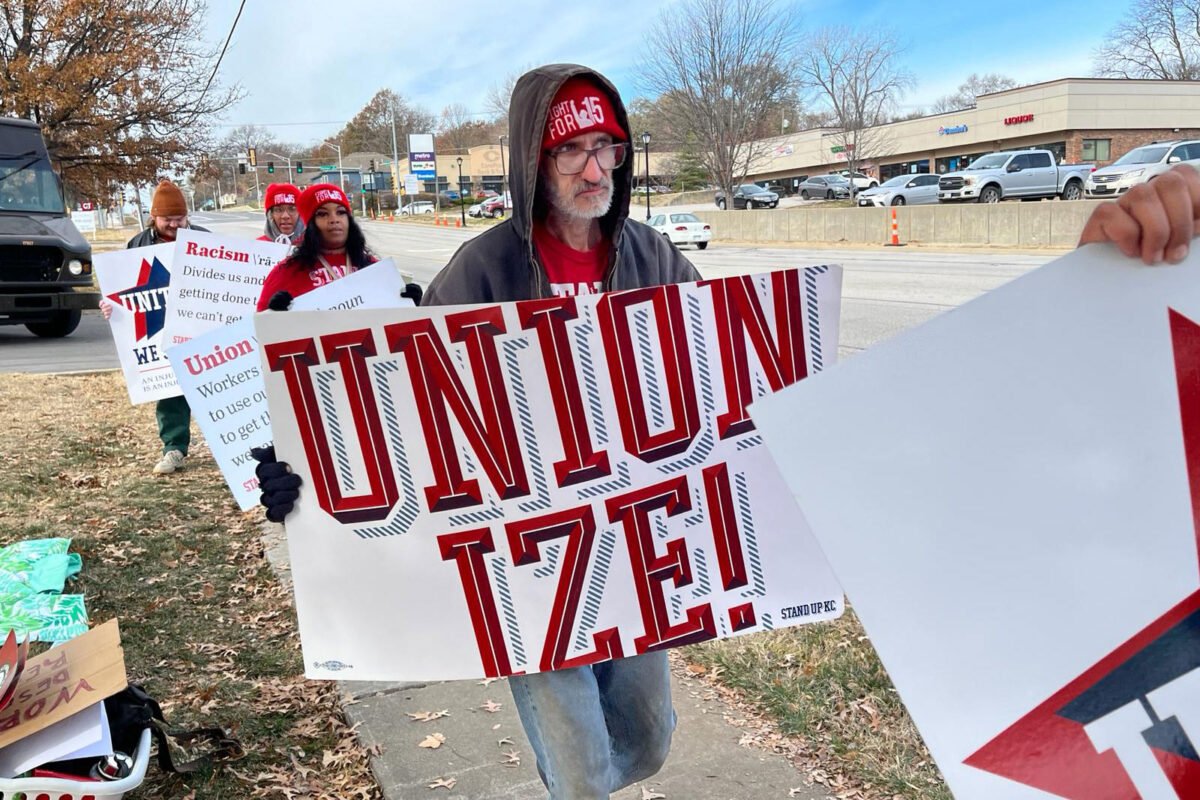
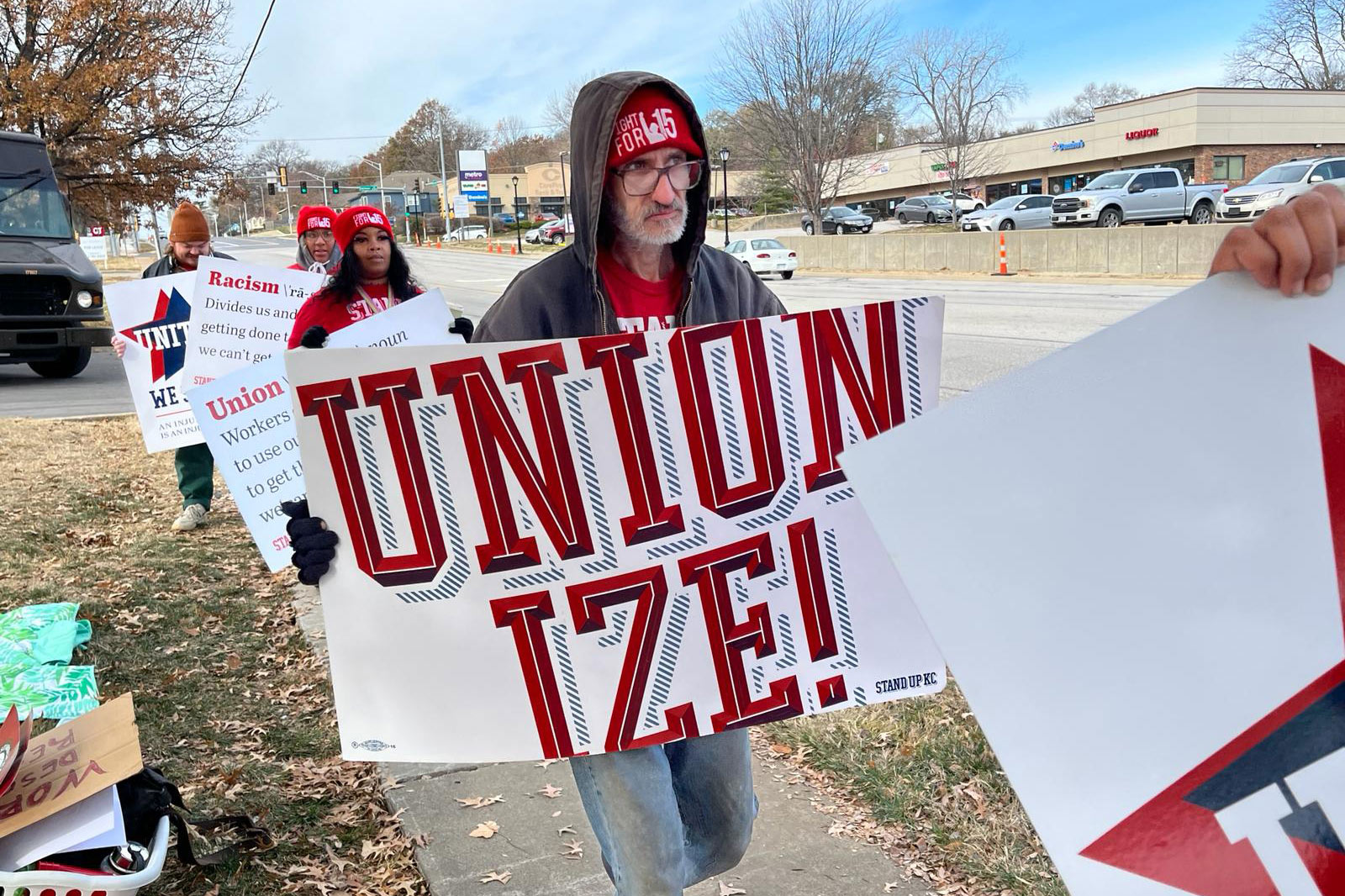
Bill Thompson’s wife had never seen him smile with confidence. For the first 20 years of their relationship, an infection in his mouth robbed him of teeth, one by one.
“I didn’t have any teeth to smile with,” the 53-year-old of Independence, Missouri, said.
Thompson said he dealt with throbbing toothaches and painful swelling in his face from abscesses for years working as a cook at Burger King. He desperately needed to see a dentist but said he couldn’t afford to take time off without pay. Missouri is one of many states that do not require employers to provide paid sick leave.
So, Thompson would swallow Tylenol and push through the pain as he worked over the hot grill.
“Either we go to work, have a paycheck,” Thompson said. “Or we take care of ourselves. We can’t take care of ourselves because, well, this vicious circle that we’re stuck in.”
In a nation that was sharply divided about government health mandates during the covid-19 pandemic, the public has been warming to the idea of government rules providing for paid sick leave.
Before the pandemic, 10 states and the District of Columbia had laws requiring employers to provide paid sick leave. Since then, Colorado, New York, New Mexico, Illinois, and Minnesota have passed laws offering some kind of paid time off for illness. Oregon and California expanded previous paid leave laws. In Missouri, Alaska, and Nebraska, advocates are pushing to put the issue on the ballot this fall.
The U.S. is one of nine countries that do not guarantee paid sick leave, according to data compiled by the World Policy Analysis Center.
In response to the pandemic, Congress passed the Emergency Paid Sick Leave and Emergency Family and Medical Leave Expansion acts. These temporary measures allowed employees to take up to two weeks of paid sick leave for covid-related illness and caregiving. But the provisions expired in 2021.
“When the pandemic hit, we finally saw some real political will to solve the problem of not having federal paid sick leave,” said economist Hilary Wething.
Subscribe to California Healthline’s free Daily Edition.
Wething co-authored a recent Economic Policy Institute report on the state of sick leave in the United States. It found that more than half, 61%, of the lowest-paid workers can’t get time off for an illness.
“I was really surprised by how quickly losing pay — because you’re sick — can translate into immediate and devastating cuts to a family’s household budget,” she said.
Wething noted that the lost wages of even a day or two can be equivalent to a month’s worth of gasoline a worker would need to get to their job, or the choice between paying an electric bill or buying food. Wething said showing up to work sick poses a risk to co-workers and customers alike. Low-paying jobs that often lack paid sick leave — like cashiers, nail technicians, home health aides, and fast-food workers — involve lots of face-to-face interactions.
“So paid sick leave is about both protecting the public health of a community and providing the workers the economic security that they desperately need when they need to take time away from work,” she said.
The National Federation of Independent Business has opposed mandatory sick leave rules at the state level, arguing that workplaces should have the flexibility to work something out with their employees when they get sick. The group said the cost of paying workers for time off, extra paperwork, and lost productivity burdens small employers.
According to a report by the National Bureau of Economic Research, once these mandates go into effect, employees take, on average, two more sick days a year than before a law took effect.
Illinois’ paid time off rules went into effect this year. Lauren Pattan is co-owner of the Old Bakery Beer Co. there. Before this year, the craft brewery did not offer paid time off for its hourly employees. Pattan said she supports Illinois’ new law but she has to figure out how to pay for it.
“We really try to be respectful of our employees and be a good place to work, and at the same time we get worried about not being able to afford things,” she said.
That could mean customers have to pay more to cover the cost, Pattan said.
As for Bill Thompson, he wrote an op-ed for the Kansas City Star newspaper about his dental struggles.
“Despite working nearly 40 hours a week, many of my co-workers are homeless,” he wrote. “Without health care, none of us can afford a doctor or a dentist.”
That op-ed generated attention locally and, in 2018, a dentist in his community donated his time and labor to remove Thompson’s remaining teeth and replace them with dentures. This allowed his mouth to recover from the infections he’d been dealing with for years. Today, Thompson has a new smile and a job — with paid sick leave — working in food service at a hotel.
In his free time, he’s been collecting signatures to put an initiative on the November ballot that would guarantee at least five days of earned paid sick leave a year for Missouri workers. Organizers behind the petition said they have enough signatures to take it before the voters.
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
Wade Trammell recalls the time he and his fellow firefighters responded to a highway crash in which a beer truck rammed into a pole, propelling the truck’s engine through the cab and into the driver’s abdomen.
“The guy was up there screaming and squirming. Then the cab caught on fire,” Trammell says. “I couldn’t move him. He burned to death right there in my arms.”
Memories of that gruesome death and other traumatic incidents he had witnessed as a firefighter in Mountain View, California, didn’t seem to bother Trammell for the first seven years after he retired in 2015. But then he started crying a lot, drinking heavily, and losing sleep. At first, he didn’t understand why, but he would later come to suspect that he was suffering from post-traumatic stress disorder.
After therapy failed to improve his mental well-being, he heard about the potential benefits of psychedelic drugs to help first responders with PTSD.
Last July, Trammell went on a retreat in Puerto Vallarta, Mexico, organized by The S.I.R.E.N. Project, a nonprofit that advocates the use of psychedelics and other alternative medicines to help first responders. He took psilocybin mushrooms and, the next day, another psychedelic derived from the toxic secretions of the Sonoran Desert toad. The experience, he says, produced an existential shift in the way he thinks of the terrible things he saw as a firefighter.
“All that trauma and all that crap I saw and dealt with, it’s all very temporary and everything goes back into the universe as energy,” Trammell says.
Wade Trammell, a former firefighter in Mountain View, California, witnessed plenty of traumatizing incidents while on the job, but it wasn’t until seven years after he retired that he felt symptoms of post-traumatic stress disorder. Last July, he attended a retreat in Mexico, at which he took psilocybin mushrooms and another psychedelic drug. He says it shifted his attitude and that he has felt better ever since.(Wade Trammell)
Abundant research has shown that psychedelics have the potential to produce lasting relief from depression, anxiety, PTSD, addiction, and other mental health conditions. Many universities around the United States have programs researching psychedelics. But experts warn that these powerful drugs are not for everybody, especially those with a history of psychosis or cardiovascular problems.
Most psychedelic drugs are prohibited under federal law, but California may soon join a growing number of local and state governments allowing their use.
SB 1012, which is working its way through the California Legislature, would allow the therapeutic use of psilocybin; mescaline; MDMA, the active ingredient in ecstasy; and dimethyltryptamine, the active ingredient in ayahuasca, a plant-based psychoactive tea. The drugs could be purchased and ingested in approved locations under the supervision of facilitators, who would undergo training and be licensed by a new state board. The facilitators would need a professional health credential to qualify.
The bill, co-sponsored by Sen. Scott Wiener (D-San Francisco), Assembly member Marie Waldron (R-San Diego), and several other lawmakers, follows last year’s unsuccessful effort to decriminalize certain psychedelics for personal use. Gov. Gavin Newsom, a Democrat, vetoed that bill, though he extolled psychedelics as “an exciting frontier” and asked for new legislation with “regulated treatment guidelines.”
Wiener says the new bill was drafted with Newsom’s request in mind. It is supported by some veterans and first responder groups and opposed by numerous law enforcement agencies.
One potential roadblock is the state’s budget deficit, which is pegged at between $38 billion and $73 billion. Newsom and legislative leaders may choose not to launch a new initiative when they are cutting existing programs. “That is something we’ll certainly grapple with,” Wiener says.
The legislation, which is making its way through committees, would require the new board to begin accepting facilitator license applications in April 2026. The system would look somewhat like the one in Oregon, which allows the use of psilocybin mushrooms under the guidance of state-licensed facilitators at psilocybin service centers. And like Oregon, California would not allow for the personal use or possession of psychedelics; the drugs would have to be purchased and consumed at the authorized locations.
Colorado, following the passage of a ballot initiative in 2022, is creating a system of regulated “healing centers,” where people will be able to legally consume psilocybin mushrooms and some other psychedelics under the supervision of licensed facilitators. Colorado’s law allows for the personal use and possession of a handful of psychedelics.
In California, the cities of Oakland, San Francisco, Berkeley, Santa Cruz, and Arcata have effectively decriminalized many psychedelics, as have other cities around the United States, including Ann Arbor, Michigan; Cambridge, Massachusetts; Detroit; Minneapolis; Seattle; and Washington, D.C.
Subscribe to California Healthline’s free Daily Edition.
Psychedelics such as psilocybin, ayahuasca, and peyote have been used for thousands of years by Indigenous populations in Latin America and the current-day United States. And some non-Indigenous groups use these substances in a spiritual way.
The Church of Ambrosia, with locations in San Francisco and Oakland, considers psilocybin mushrooms, also known as magic mushrooms, a sacrament. “Mushrooms affect the border between this world and the next, and allow people to connect to their soul,” says Dave Hodges, founder and pastor of the church.
Hodges was behind an unsuccessful attempt to get an initiative on the California ballot this year that would have decriminalized the possession and use of mushrooms. He hopes it will qualify for the 2026 ballot.
The pending California legislation is rooted in studies showing psychedelics can be powerful agents in mental health treatment.
Charles Grob, a psychiatry professor at the University of California-Los Angeles School of Medicine who has researched psychedelics for nearly 40 years, led a study that found synthetic psilocybin could help reduce end-of-life anxiety in patients with advanced-stage cancer.
Grob says that MDMA is good for couples counseling because it facilitates communication and puts people in touch with their feelings. And he conducted research in Brazil that showed ayahuasca used in a religious context helped people overcome alcoholism.
But Grob warns that the unsupervised use of psychedelics can be dangerous and says people should undergo mental and medical health screenings before ingesting them. “There are cases of people going off the rails. It’s a small minority, but it can happen and when it does happen it can be very frightening,” Grob says.
Ken Finn, past president of the American Board of Pain Medicine, says psychedelics have a number of side effects, including elevated blood pressure, high heart rate, and vomiting, and that they can trigger “persistent psychosis” in a small minority of users. Legal drugs also pose risks, he says, “but we have much better guardrails on things like prescriptions and over-the-counter medications.” He also worries about product contamination and says manufacturers would need to be tightly regulated.
Another potential problem is health equity. Since insurance would not cover these sessions, at least initially, they would likely attract people with disposable income. A supervised psilocybin journey in Oregon, for example, can cost more than $2,500.
Many people who have experienced psychedelics corroborate the research results. Ben Kramer, a former Marine who served in Afghanistan and now works as a psilocybin facilitator in Beaverton, Oregon, says a high-dose mushroom session altered his worldview.
“I relived the first time I was ever shot at in Afghanistan,” he says. “I was there. I had this overwhelming love and compassion for the guy who was shooting at me, who was fighting for what he believed in, just like I was.”
Another characteristic of psychedelic therapy is that just a few sessions can potentially produce lasting results.
Trammell, the retired firefighter, hasn’t taken psychedelics since that retreat in Mexico 10 months ago. “I just felt like I kind of got what I needed,” he says. “I’ve been fine ever since.”
James Lemons, 39, wants the bullet removed from his thigh so he can go back to work.
Sarai Holguin, a 71-year-old woman originally from Mexico, has accepted the bullet lodged near her knee as her “compa” — a close friend.
Mireya Nelson, 15, was hit by a bullet that went through her jaw and broke her shoulder, where fragments remain. She’ll live with them for now, while doctors monitor lead levels in her blood for at least two years.
Nearly three months after the Kansas City Chiefs Super Bowl parade shooting left at least 24 people injured, recovery from those wounds is intensely personal and includes a surprising gray area in medicine: whether the bullets should be removed.
Medical protocol offers no clear answer. A 2016 survey of surgeons found that only about 15% of respondents worked at medical facilities that had policies on bullet removal. Doctors in the U.S. often leave bullets buried deep in a person’s body, at least at first, so as not to cause further trauma.
But as gun violence has emerged as a public health epidemic, some researchers wonder if that practice is best. Some of the wounded, like James Lemons, are left in a precarious place.
“If there’s a way to get it out, and it’s safely taken out, get it out of the person,” Lemons said. “Make that person feel more secure about themselves. And you’re not walking around with that memory in you.”
Lemons, Holguin, and Nelson are coping in very different ways.
Pain Became a Problem
Three days after the Chiefs won the Super Bowl, Lemons drove the 37 miles from Harrisonville, Missouri, to downtown Kansas City to celebrate the victory. The warehouse worker was carrying his 5-year-old daughter, Kensley, on his shoulders when he felt a bullet enter the back of his right thigh.
James Lemons was carrying daughter Kensley on his shoulders at the Kansas City Chiefs Super Bowl parade when he felt a bullet enter the back of his right thigh. He says his first thought amid the chaos was getting his family to safety.(Brandie Lemons)
Gunfire erupted in the area packed with revelers, prosecutors later said, after a “verbal confrontation” between two groups. Detectives found “multiple 9mm and .40 caliber spent shell casings” at the scene. Lemons said he understood immediately what was happening.
“I know my city. We’re not shooting off fireworks,” he said.
Lemons shielded Kensley’s face as they fell to the ground so she wouldn’t hit the concrete. His first thought was getting his family — also including his wife, Brandie; 17-year-old daughter, Kallie; and 10-year-old son, Jaxson — to safety.
“I’m hit. But don’t worry about it,” Lemons recalled telling Brandie. “We gotta go.”
He carried Kensley on his shoulders as the family walked a mile to their car. His leg bled through his pants at first then stopped, he said. It burned with pain. Brandie insisted on driving him to the hospital but traffic was at a standstill so she put on her hazard lights and drove on the wrong side of the road.
“She’s like: ‘I’m getting you to a hospital. I’m tired of people being in my way,’” Lemons recalled. “I’ve never seen my wife like that. I’m looking at her like, ‘That’s kinda sexy.’”
Lemons clapped and smiled at his wife, he said, to which she replied, “What are you smiling for? You just got shot.” He stayed in quiet admiration until they were stopped by a sheriff, who summoned an ambulance, Lemons said.
He was taken to the emergency room at University Health, which admitted 12 patients from the rally, including eight with gunshot wounds. Imaging showed the bullet barely missed an artery, Lemons said. Doctors cleansed the wound, put his leg in a brace, and told him to come back in a week. The bullet was still in his leg.
“I was a little baffled by it, but I was like, ‘OK, whatever, I’ll get out of here,’” Lemons recalled.
When he returned, doctors removed the brace but explained they often leave bullets and fragments in the body — unless they grow too painful.
“I get it, but I don’t like that,” Lemons said. “Why wouldn’t you take it out if you could?”
University Health spokesperson Leslie Carto said the hospital can’t comment on individual patient care because of federal privacy laws.
Subscribe to California Healthline’s free Daily Edition.
Surgeons typically do remove bullets when they encounter them during surgery or they are in dangerous locations, like in the spinal canal or risking damage to an organ, said Brendan Campbell, a pediatric surgeon at Connecticut Children’s.
Campbell also chairs the Injury Prevention and Control Committee of the American College of Surgeons’ Committee on Trauma, which works on firearm injury prevention.
LJ Punch, a trauma surgeon by training and the founder of the Bullet Related Injury Clinic in St. Louis, said the origins of trauma care also help explain why bullets are so often left.
“Trauma care is war medicine,” Punch said. “It is set to be ready at any moment and any time, every day, to save a life. It is not equipped to take care of the healing that needs to come after.”
In the survey of surgeons, the most common reasons given for removing a bullet were pain, a palpable bullet lodged near the skin, or an infection. Far less common were lead poisoning and mental health concerns such as post-traumatic stress disorder and anxiety.
What patients wanted also affected their decisions, the surgeons said.
After being shot in the leg at the Kansas City Chiefs Super Bowl parade, Lemons was initially told the bullet would stay there, unless it became a problem. “I get it, but I don’t like that,” Lemons says. “Why wouldn’t you take it out if you could?”(Bram Sable-Smith/KFF Health News)
Lemons wanted the bullet out. The pain it caused in his leg radiated up from his thigh, making it difficult to move for more than an hour or two. Working his warehouse job was impossible.
“I gotta lift 100 pounds every night,” Lemons recalled telling his doctors. “I gotta lift my child. I can’t work like this.”
He has lost his income and his health insurance. Another stroke of bad luck: The family’s landlord sold their rental home soon after the parade, and they had to find a new place to live. This house is smaller, but it was important to keep the kids in the same school district with their friends, Lemons said in an interview in Kensley’s pink bedroom, the quietest spot to talk.
They’ve borrowed money and raised $6,500 on GoFundMe to help with the deposit and car repairs, but the parade shooting has left the family in a deep financial hole.
Without insurance, Lemons worried he couldn’t afford to have the bullet removed. Then he learned his surgery would be paid for by donations. He set up an appointment at a hospital north of the city, where a surgeon took measurements on his X-ray and explained the procedure.
“I need you to be involved as much as I’m going to be involved,” he remembered being told, “because — guess what — this ain’t my leg.”
The surgery is scheduled for this month.
‘We Became Friends’
Sarai Holguin isn’t much of a Chiefs fan, but she agreed to go to the rally at Union Station to show her friend the best spot to see the players on stage. It was an unseasonably warm day, and they were standing near an entrance where lots of police were stationed. Parents had babies in strollers, kids were playing football, and she felt safe.
A little before 2 p.m., Holguin heard what she thought were fireworks. People started running away from the stage. She turned to leave, trying to find her friend, but felt dizzy. She didn’t know she’d been shot. Three people quickly came to her aid and helped her to the ground, and a stranger took off his shirt and made a tourniquet to put on her left leg.
Holguin, a native of Puebla, Mexico, who became a U.S. citizen in 2018, had never seen so much chaos, so many paramedics working under such pressure. They were “anonymous heroes,” she said.
She saw them working on Lisa Lopez-Galvan, a well-known DJ and 43-year-old mother of two. Lopez-Galvan died at the scene, and was the sole fatality at the parade. Holguin was rushed to University Health, about five minutes from Union Station.
In the chaos of being shot at the Kansas City Chiefs Super Bowl parade, then hospitalized, Sarai Holguin lost her purse and cellphone. Her husband, Cesar, and daughter searched for her for about eight hours.(Christopher Smith for KFF Health News)
There doctors performed surgery, leaving the bullet in her leg. Holguin awoke to more chaos. She had lost her purse, along with her cellphone, so she couldn’t call her husband, Cesar. She had been admitted to the hospital under an alias — a common practice at medical centers to begin immediate care.
Her husband and daughter didn’t find her until about 10 p.m. — roughly eight hours after she’d been shot.
“It has been a huge trauma for me,” Holguin said through an interpreter. “I was injured and at the hospital without doing anything wrong. [The rally] was a moment to play, to relax, to be together.”
Holguin was hospitalized for a week, and two more outpatient surgeries quickly followed, mostly to remove dead tissue around the wound. She wore a wound VAC, or vacuum-assisted closure device, for several weeks and had medical appointments every other day.
Campbell, the trauma surgeon, said wound VACs are common when bullets damage tissue that isn’t easily reconstructed in surgery.
“It’s not just the physical injuries,” Campbell said. “Many times it’s the emotional, psychological injuries, which many of these patients take away as well.”
The bullet remains near Holguin’s knee.
Holguin, a native of Puebla, Mexico, who became a U.S. citizen in 2018, was shot in the leg at the Kansas City Chiefs Super Bowl parade. Now using a walker, she says the most frustrating consequence is not being able to travel to see her father, still in Mexico.(Christopher Smith for KFF Health News)
“I’m going to have it for the rest of my life,” she said, saying she and the bullet became “compas,” close friends.
“We became friends so that she doesn’t do any bad to me anymore,” Holguin said with a smile.
Punch, of the Bullet Related Injury Clinic in St. Louis, said some people like Holguin are able to find a way to psychically live with bullets that remain.
“If you’re able to make a story around what that means for that bullet to be in your body, that gives you power; that gives you agency and choice,” Punch said.
Holguin’s life changed in an instant: She’s using a walker to get around. Her foot, she said, acts “like it had a stroke” — it dangles, and it’s difficult to move her toes.
The most frustrating consequence is that she cannot travel to see her 102-year-old father, still in Mexico. She has a live camera feed on her phone to see him, but that doesn’t offer much comfort, she said, and thinking about him brings tears.
She was told at the hospital that her medical bills would be taken care of, but then lots of them came in the mail. She tried to get victim assistance from the state of Missouri, but all the forms she had were in English, which made them difficult to comprehend. Renting the wound VAC alone cost $800 a month.
Finally she heard that the Mexican Consulate in Kansas City could help, and the consul pointed her to the Jackson County Prosecutor’s Office, with which she registered as an official victim. Now all of her bills are being paid, she said.
Holguin isn’t going to seek mental health treatment, as she believes one must learn to live with a given situation or it will become a burden.
“I have processed this new chapter in my life,” Holguin said. “I have never given up and I will move on with God’s help.”
At the Kansas City Chiefs Super Bowl parade, Holguin heard what she thought were fireworks, unaware she had been shot. She underwent surgery and doctors opted to leave the bullet in her leg. She’s now using a walker to get around.(Christopher Smith for KFF Health News)
‘I Saw Blood on My Hands’
Mireya Nelson was late to the parade. Her mother, Erika, told her she should leave early, given traffic and the million people expected to crowd into downtown Kansas City, but she and her teenage friends ignored that advice. The Nelsons live in Belton, Missouri, about a half hour south of the city.
Mireya wanted to hold the Super Bowl trophy. When she and her three friends arrived, the parade that had moved through downtown was over and the rally at Union Station had begun. They were stuck in the large crowd and quickly grew bored, Mireya said.
Getting ready to leave, Mireya and one of her friends were trying to call the driver of their group, but they couldn’t get cell service in the large crowd.
Amid the chaos of people and noise, Mireya suddenly fell.
A bullet went through the jaw of Mireya Nelson during the Kansas City Chiefs Super Bowl parade on Feb. 14. She also has bullet fragments in her shoulder and will need to have her blood tested for lead for at least the next two years.(Erika Nelson)
“I saw blood on my hands. So then I knew I got shot. Yeah, and I just crawled to a tree,” Mireya said. “I actually didn’t know where I got shot at, at first. I just saw blood on my hands.”
The bullet grazed Mireya’s chin, shot through her jaw, broke her shoulder, and left through her arm. Bullet fragments remain in her shoulder. Doctors decided to leave them because Mireya had already suffered so much damage.
Mireya’s mother supports that decision, for now, noting they were just “fragments.”
“I think if it’s not going to harm her the rest of her life,” Erika said, “I don’t want her to keep going back in the hospital and getting surgery. That’s more trauma to her and more recovery time, more physical therapy and stuff like that.”
Bullet fragments, particularly ones only skin-deep, often push their way out like splinters, according to Punch, although patients aren’t always told about that. Moreover, Punch said, injuries caused by bullets extend beyond those with damaged tissue to the people around them, like Erika. He called for a holistic approach to recover from all the trauma.
“When people stay in their trauma, that trauma can change them for a lifetime,” Punch said.
Mireya will be tested for lead levels in her blood for at least the next two years. Her levels are fine now, doctors told the family, but if they get worse she will need surgery to remove the fragments, her mother said.
Campbell, the pediatric surgeon, said lead is particularly concerning for young children, whose developing brains make them especially vulnerable to its harmful effects. Even a tiny amount of lead — 3.5 micrograms per deciliter — is enough to report to state health officials, according to the Centers for Disease Control and Prevention.
Nelson was one of at least 24 people injured by gunfire during the parade. Here, Chiefs quarterback Patrick Mahomes and his wife, Brittany, visit her at Children’s Mercy hospital.(Erika Nelson)
Mireya talks about cute teenage boys’ being “fine” but also still wears Cookie Monster pajamas. She appears confused by the shootings, by all the attention at home, at school, from reporters. Asked how she feels about the fragments in her arm, she said, “I don’t really care for them.”
Mireya was on antibiotics for 10 days after her hospital stay because doctors feared there was bacteria in the wound. She has had physical therapy, but it’s painful to do the exercises. She has a scar on her chin. “A dent,” she said, that’s “bumpy.”
“They said she was lucky because if she wouldn’t have turned her head in a certain way, she could be gone,” Erika said.
Mireya faces a psychiatric evaluation and therapy appointments, though she doesn’t like to talk about her feelings.
So far, Erika’s insurance is paying the medical bills, though she hopes to get some help from the United Way’s #KCStrong fund, which raised nearly $1.9 million, or a faith-based organization called Unite KC.
Erika doesn’t want a handout. She has a job in health care and just got a promotion.
The bullet has changed the family’s life in big ways. It is part of their conversation now. They talk about how they wish they knew what kind of ammunition it was, or what it looked like.
“Like, I wanted to keep the bullet that went through my arm,” Mireya said. “I want to know what kind of bullet it was.” That brought a sigh from her mom, who said her daughter had watched too many episodes of “Forensic Files.”
Erika beats herself up about the wound, because she couldn’t protect her daughter at the parade.
“It hits me hard because I feel bad because she begged me to get off work and I didn’t go there because when you have a new position, you can’t just take off work,” Erika said. “Because I would have took the bullet. Because I would do anything. It’s mom mode.”
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
HOUSTON — Patients admitted to Houston Methodist Hospital get a monitoring device about the size of a half-dollar affixed to their chest — and an unwitting role in the expanding use of artificial intelligence in health care.
The slender, battery-powered gadget, called a BioButton, records vital signs including heart and breathing rates, then wirelessly sends the readings to nurses sitting in a 24-hour control room elsewhere in the hospital or in their homes. The device’s software uses AI to analyze the voluminous data and detect signs a patient’s condition is deteriorating.
Hospital officials say the BioButton has improved care and reduced the workload of bedside nurses since its rollout last year.
“Because we catch things earlier, patients are doing better, as we don’t have to wait for the bedside team to notice if something is going wrong,” said Sarah Pletcher, system vice president at Houston Methodist.
But some nurses fear the technology could wind up replacing them rather than supporting them — and harming patients. Houston Methodist, one of dozens of U.S. hospitals to employ the device, is the first to use the BioButton to monitor all patients except those in intensive care, Pletcher said.
“The hype around a lot of these devices is they provide care at scale for less labor costs,” said Michelle Mahon, a registered nurse and an assistant director of National Nurses United, the profession’s largest U.S. union. “This is a trend that we find disturbing,” she said.
The rollout of BioButton is among the latest examples of hospitals deploying technology to improve efficiency and address a decades-old nursing shortage. But that transition has raised its own concerns, including about the device’s use of AI; polls show the public is wary of health providers relying on it for patient care.
The BioButton, a monitoring device, is being used in dozens of hospitals employing artificial intelligence to analyze patients’ vital signs. (Phil Galewitz/KFF Health News)
Houston Methodist Hospital, just a few miles south of downtown Houston, is located amid a giant medical complex that includes several hospitals. (Phil Galewitz/KFF Health News)
In December 2022 the FDA cleared the BioButton for use in adult patients who are not in critical care. It is one of many AI tools now used by hospitals for tasks like reading diagnostic imaging results.
In 2023, President Joe Biden directed the Department of Health and Human Services to develop a plan to regulate AI in hospitals, including by collecting reports of patients harmed by its use.
The leader of BioIntelliSense, which developed the BioButton, said its device is a huge advance compared with nurses walking into a room every few hours to measure vital signs. “With AI, you now move from ‘I wonder why this patient crashed’ to ‘I can see this crash coming before it happens and intervene appropriately,’” said James Mault, CEO of the Golden, Colorado-based company.
The BioButton stays on the skin with an adhesive, is waterproof, and has up to a 30-day battery life. The company says the device — which allows providers to quickly notice deteriorating health by recording more than 1,000 measurements a day per patient — has been used on more than 80,000 hospital patients nationwide in the past year.
Hospitals pay BioIntelliSense an annual subscription fee for the devices and software.
Houston Methodist officials would not reveal how much the hospital pays for the technology, though Pletcher said it equates to less than a cup of coffee a day per patient.
For a hospital system that treats thousands of patients at a time — Houston Methodist has 2,653 non-ICU beds at its eight Houston-area hospitals — such an investment could still translate to millions of dollars a year.
Subscribe to California Healthline’s free Daily Edition.
Hospital officials say they have not made any changes in nurse staffing and have no plans to because of implementing the BioButton.
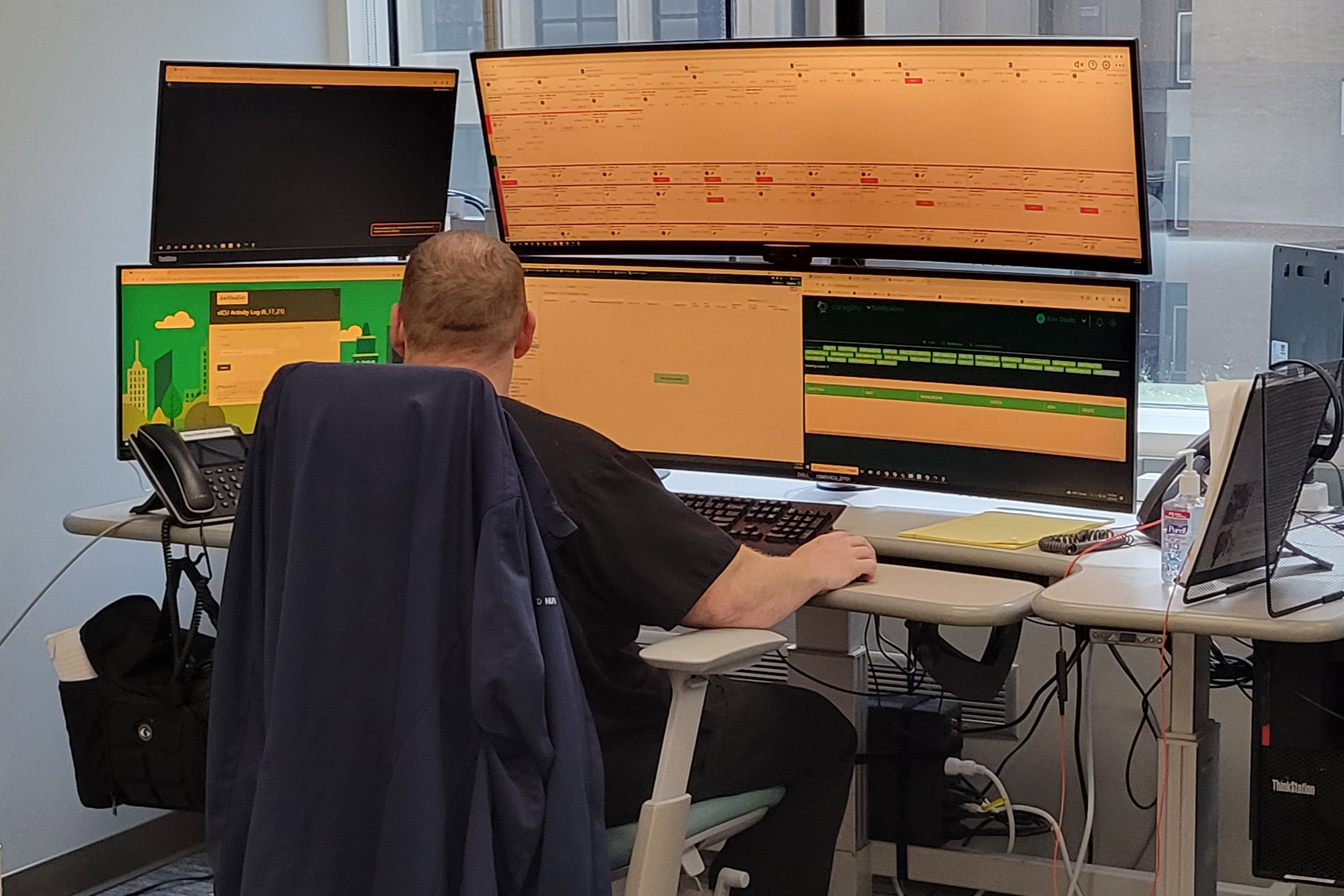
Inside the hospital’s control center for virtual monitoring on a recent morning, about 15 nurses and technicians dressed in scrubs sat in front of large monitors showing the health status of hundreds of patients they were assigned to monitor.
A red checkmark next to a patient’s name signaled the AI software had found readings trending outside normal. Staff members could click into a patient’s medical record, showing patients’ vital signs over time and other medical history. These virtual nurses, if you will, could contact nurses on the floor by phone or email, or even dial directly into the patient’s room via video call.
Nutanben Gandhi, a technician who was watching 446 patients on her monitor that morning, said that when she gets an alert, she looks at the patient’s health record to see if the anomaly can be easily explained by something in the patient’s condition or if she needs to contact nurses on the patient’s floor.
Oftentimes an alert can be easily dismissed. But identifying signs of deteriorating health can be tough, said Steve Klahn, Houston Methodist’s clinical director of virtual medicine.
“We are looking for a needle in a haystack,” he said.
Donald Eustes, 65, was admitted to Houston Methodist in March for prostate cancer treatment and has since been treated for a stroke. He is happy to wear the BioButton.
“You never know what can happen here, and having an extra set of eyes looking at you is a good thing,” he said from his hospital bed. After being told the device uses AI, the Montgomery, Texas, man said he has no problem with its helping his clinical team. “This sounds like a good use of artificial intelligence.”
Patients and nurses alike benefit from remote monitoring like the BioButton, said Pletcher of Houston Methodist.
A nurse inside Houston Methodist Hospital’s virtual intensive care unit monitors patients from afar. Nurses can track dozens of patients using technology that helps them supplement bedside care. (Phil Galewitz/KFF Health News)
Sarah Pletcher, system vice president at Houston Methodist, stands inside the hospital’s 24-hour virtual intensive care unit where patients are monitored by nurses and technicians. (Phil Galewitz/KFF Health News)
The hospital has placed small cameras and microphones inside all patient rooms enabling nurses outside to communicate with patients and perform tasks such as helping with patient admissions and discharge instructions. Patients can include family members on the remote calls with nurses or a doctor, she said.
Virtual technology frees up on-duty nurses to provide more hands-on help, such as starting an intravenous line, Pletcher said. With the BioButton, nurses can wait to take routine vital signs every eight hours instead of every four, she said.
Pletcher said the device reduces nurses’ stress in monitoring patients and allows some to work more flexible hours because virtual care can be done from home rather than coming to the hospital. Ultimately it helps retain nurses, not drive them away, she said.
Sheeba Roy, a nurse manager at Houston Methodist, said some members of the nursing staff were nervous about relying on the device and not checking patients’ vital signs as often themselves. But testing has shown the device provides accurate information.
“After we implemented it, the staff loves it,” Roy said.
Houston Methodist this year plans to send the BioButton home with patients so the hospital can better track their progress in the weeks after discharge, measuring the quality of their sleep and checking their gait.(Phil Galewitz/KFF Health News)
Serena Bumpus, chief executive officer of the Texas Nurses Association, said her concern with any technology is that it can be more burdensome on nurses and take away time with patients.
“We have to be hypervigilant in ensuring that we are not leaning on this to replace the ability of nurses to critically think and assess patients and validate what this device is telling us is true,” Bumpus said.
Houston Methodist this year plans to send the BioButton home with patients so the hospital can better track their progress in the weeks after discharge, measuring the quality of their sleep and checking their gait.
“We are not going to need less nurses in health care, but we have limited resources and we have to use those as thoughtfully as we can,” Pletcher said. “Looking at projected demand and seeing the supply we have coming, we will not have enough to meet demand, so anything we can do to give time back to nurses is a good thing.”
This article was produced by KFF Health News, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
Newswise — COLUMBUS, Ohio – Rural Americans are less likely to initiate care for substance use disorders and to receive ongoing care compared with those who live in urban areas, according to a new study.
When they do access care, people who live in less populated areas are more likely to have to go outside their provider network to receive treatment, which comes with higher out-of-pocket costs, found a team of researchers at The Ohio State University College of Public Health. Their study appears in the journal Health Services Research.
“One thing that’s really striking is that we looked at sort of a best-case scenario for people with substance use disorders – care for people with private insurance tends to include high reimbursement rates and specialists are more likely to contract with those plans, meaning they have more robust provider networks,” said study lead author Eli Raver, an Ohio State doctoral student.
“If we find problems among this group, you know it’s going to be worse for everybody else.”
Looking at an employer-sponsored health care database, the research team examined data collected from 2016 through 2018 that included about 40 million adult patients each year.
Treatment rates for substance use disorders were low across the board – less than half of people received care. But the picture was worse for rural Americans.
Among the disparities found in the study:
Rural patients experienced lower treatment initiation rates for disorders involving alcohol (37% vs. 38%), opioids (41% vs. 44%) and other drugs (38% vs. 40%) compared to those in urban areas.
Rural patients were also less likely than urban patients to engage in ongoing treatment for alcohol (15% vs. 17%), opioids (21% vs. 23%) and other drugs (16% vs. 18%).
More rural patients than urban patients received out-of-network initial treatment and continued treatment for drug use disorders other than alcohol and opioids. Rural patients were also more likely to pay higher rates for ongoing treatment for alcohol use disorders.
While substance use disorders and struggles finding and completing successful treatment are widespread concerns, matters are worse for those who live in rural areas, and this new research contributes more understanding about the obstacles people face, said Wendy Xu, the study’s senior author and an associate professor of health services management and policy at Ohio State.
“Rural areas are continuously plagued with a shortage of behavioral health providers and more limited health resources overall. These challenges are compounded by the fact that most insurance plans use managed care arrangements, some of which use highly limited provider networks,” Xu said.
One potential approach to tackling these problems could be the Collaborative Care Model, which has grown in popularity in recent years, she said: “This model allows primary care clinicians working with a behavioral health care manager, who often is not an advanced clinician, to treat substance use disorders in collaboration with a psychiatric consultant who doesn’t have to live and work in the area.”
In fact, the entire collaborative process of treatments, prescribing and ongoing care are typically delivered through virtual health appointments and billed through the patient’s primary care practice.
Raver said it’s important to note that while much of policymakers’ attention is focused on opioid use disorders, the disparities identified in this study exist across the spectrum of substance use disorders.
“A lot of policy focus has been on the opioid crisis, as it should be, but I think it’s interesting and troubling to see that, regardless of which substance we’re talking about, there is high out-of-network usage and low overall participation in care,” he said.
Study co-authors include Sheldon Retchin of Ohio State, Yiting Li of Nationwide Children’s Hospital and Andrew Carlo of Northwestern University.
Newswise — A growing number of states and territories in the United States have legalized medical and recreational cannabis use. As such, recreational cannabis has been associated with a lower perception of risk of harm in the general U.S. population.
However, in women of childbearing age, evidence has shown that cannabis use may increase the risk of adverse reproductive and perinatal health outcomes. Furthermore, research on the perception of risk from using cannabis among vulnerable populations such as those with disabilities is lacking.
Using data from the 2021 National Survey on Drug Use and Health, researchers from Florida Atlantic University’s Schmidt College of Medicine conducted a study to assess the perceived risk of harm associated with weekly cannabis use in a sample of 20,234 women ages 18 to 49 by disability status.
Disabilities included sensory (hearing and vision), cognitive (difficulty remembering and concentrating) and daily activities (e.g., walking and self-care). Researchers included race/ethnicity, age, marital status, federal poverty level, past-year health insurance gap, and whether the state of residence legalized medical cannabis. They also assessed perceived overall health status, past-year major depressive episode, past-month tobacco/alcohol use, and illicit drug use.
Results of the study, published in the journal Cannabis and Cannabinoid Research, showed that approximately 60% of women with disabilities who used cannabis in the past 12 months perceived no risk of harm from weekly cannabis use. A significantly higher percentage of women with any disability perceived no risk associated with weekly cannabis use (37.9%) compared to those with no disabilities (26.1%).
More than one-quarter (27.4%) of women perceived no risk of harm associated with weekly cannabis use. Overall, perceiving no risk associated with weekly cannabis use was evident among women ages 21 to 29 (34.4%), those who were never married (32%), were non-Hispanic Black (32.2%), living in poverty (31%), perceiving their health as fair/poor (35.1%), and experienced a past 12-month major depressive episode (36.4%). The likelihood of perceiving no risk also was higher among women using tobacco and those using both alcohol and tobacco.
“Given women’s attitudes toward cannabis as a harmless drug, the increasing rates of its use among those with disabilities, and the potential adverse health outcomes, it is imperative to monitor and understand perceptions of risk of harm from cannabis use among women with disabilities,” said Panagiota “Yiota” Kitsantas, Ph.D., senior author, professor and chair, Department of Population Health and Social Medicine, FAU Schmidt College of Medicine.
Overall, women with disabilities and cannabis use in the past 12 months had 2.9 times higher odds of perceiving no risk associated with weekly use of cannabis compared to women without any disability and no cannabis use. The odds also were higher for those who did not have a disability but used cannabis in the past year, which indicates that cannabis exposure, in general, may increase a woman’s likelihood of not perceiving any harm to her health from weekly use.
Exposure to cannabis use during pregnancy has been associated with adverse birth outcomes including low birth weight, preterm delivery, small for gestational age, admission to the neonatal intensive care unit and infant death. Cannabis use also may affect sex hormones essential to fertility and the timing of ovulation in reproductive age.
“As legalization of cannabis use becomes more prevalent across states, attitudes regarding the risk of cannabis use are changing,” said Lea Sacca, Ph.D., co-author and an assistant professor in the Department of Population Health and Social Medicine, FAU Schmidt College of Medicine. “A multi-pronged approach to address cannabis use among vulnerable populations such as women of childbearing age with disabilities will require clinical guidance, provider and patient education and evidence-based public health programs.”
Although research evidence shows that residents in states where cannabis is legal are more likely to believe that cannabis has benefits than those living in states with just medically legal cannabis or nonlegal states, this study suggests that living in a state that has legalized medical cannabis was associated with a decreased likelihood of perceiving no risk from using weekly cannabis relative to states with no legalized use of medical cannabis.
“There is an urgent need for effective cannabis screening and subsequent dissuasion of cannabis use for reproductive-aged women at risk of substance use. Obstetrician-gynecologists can play an important role by informing patients about healthy behaviors and encouraging long-term adoption as well as identifying patients abusing drugs for proper referral to addiction treatment professionals,” said Kitsantas. “Importantly, health policies should include holistic programs to proactively educate the population, pharmacists, medical and public health professionals of the associated benefits and risks of cannabis use among reproductive-aged women with disabilities.”
Study co-author is Salman M. Aljoudi, a health data analyst, a Ph.D. researcher and an instructor at George Mason University.
– FAU –
About the Charles E. Schmidt College of Medicine:
FAU’s Charles E. Schmidt College of Medicine is one of approximately 157 accredited medical schools in the U.S. The college was launched in 2010, when the Florida Board of Governors made a landmark decision authorizing FAU to award the M.D. degree. After receiving approval from the Florida legislature and the governor, it became the 134th allopathic medical school in North America. With more than 70 full and part-time faculty and more than 1,300 affiliate faculty, the college matriculates 64 medical students each year and has been nationally recognized for its innovative curriculum. To further FAU’s commitment to increase much needed medical residency positions in Palm Beach County and to ensure that the region will continue to have an adequate and well-trained physician workforce, the FAU Charles E. Schmidt College of Medicine Consortium for Graduate Medical Education (GME) was formed in fall 2011 with five leading hospitals in Palm Beach County. The Consortium currently has five Accreditation Council for Graduate Medical Education (ACGME) accredited residencies including internal medicine, surgery, emergency medicine, psychiatry, and neurology.
About Florida Atlantic University: Florida Atlantic University, established in 1961, officially opened its doors in 1964 as the fifth public university in Florida. Today, the University serves more than 30,000 undergraduate and graduate students across six campuses located along the southeast Florida coast. In recent years, the University has doubled its research expenditures and outpaced its peers in student achievement rates. Through the coexistence of access and excellence, FAU embodies an innovative model where traditional achievement gaps vanish. FAU is designated a Hispanic-serving institution, ranked as a top public university by U.S. News & World Report and a High Research Activity institution by the Carnegie Foundation for the Advancement of Teaching. For more information, visit www.fau.edu.